PURPOSE: The aim of this study is to evaluate
and compare the strains generated by short and
conventional implants supporting a distal extension
removable partial overdenture under axial and
oblique loading.
MATERIALS AND METHODS: A mandibular
photoelastic resin model was printed based on
a computed tomography scan of a patient with
bilaterally missing mandibular posterior teeth. Two
implants were placed- short (4.3x6mm) on the right
side and conventional (4.3x10mm) on the left side
second molar region. A conventional Kennedy’s
Class I implant retained RPD was fabricated.
Maximum static loads of 100 N were applied in both
vertical and 45 ooblique directions in the second
molar region of the denture. Ten tests were done for
each group. The stress values around the implants
were derived from the colored fringe patterns that
were photographed after the load applications
from which strain values were derived. Data were
analyzed by unpaired t-test.
RESULTS: In both conventional and short implants,
the strains around the neck of the implants were
more on oblique loading compared to axial loading.
Comparison of average compressive strain under
axial and oblique loading showed no significant
difference between conventional and short implants.
INTERPRETATION & CONCLUSION: 1) There is no
statistically significant difference between the strains
generated by conventional and short implants under
vertical loading and oblique loading
2) The generated strains were more under oblique
loading compared to axial loading.
Key words: conventional; short; overdenture; strain; photoelasticity
Implants have revolutionized dental practice and
have helped overcome many of the limitations
encountered with conventional fixed or removable
prostheses and is considered as an aesthetic and
functional restoration.
Placing two implant abutments distally in the
mandible has been recommended to transform
a bilateral distal extension (Kennedy’s Class I)
RPD to a tooth and implant-supported/assisted
RPD (a pseudo-Kennedy’s Class III). The pseudo-Kennedy’s Class III design will improve the support,
stability, and retention of a distal extension RPD. This could be seen as a cost-effective alternative
compared to implant-retained fixed prosthetic
options1, 2.
Not all patients have sufficient bone height in
the posterior region and are often disinclined
to submit themselves to invasive surgeries prior
to the placement of the implants. These include
bone-grafting procedures in the region, or even
nerve lateralization of the inferior alveolar nerve,
which may also result in permanent paresthesia3.
An alternative is the use of short implants4,5.
Conventional implants are the preferred option
for any prosthesis. But in compromised situations
usage of short implants can be beneficial compared
to surgical corrections. Investigations on the use of
short implants have led to diverse results, and the choice remains controversial. This in-vitro study
proposed to evaluate and compare the strains
generated by short and conventional implants
supporting distal extension removable partial
overdenture in order to help the clinician make
the right choice and achieve long-term clinical
success6.
A real-life arrangement comprising of a mandibular
model was made using C-51(3222) resin and K-6
hardener employing Fused Deposition Modelling
based on a computed tomographic scan of a
patient with bilaterally missing mandibular
posterior teeth. Soft tissue was duplicated using
Gingifast- Elastic.
One short (4.3x6mm) and one conventional
(4.3x10mm) titanium tapered threaded implants
(JD Evolutions) were placed on the right and left
sides respectively in the second molar region of
the photoelastic model with an osteotomy kit, using
a standard protocol.
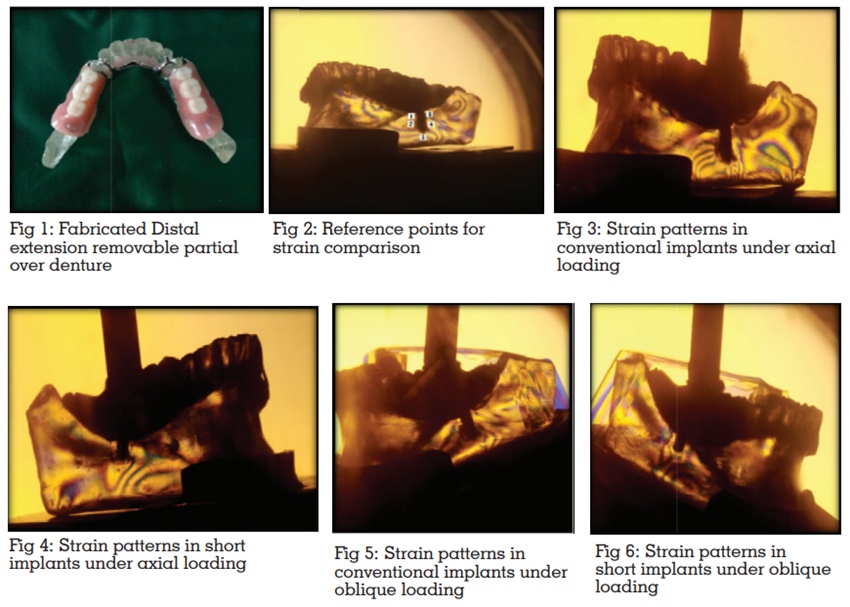
A conventional Kennedy’s Class I RPD with a
lingual bar (0.5 mm), mesial rests with canine
extensions (indirect retainers) and I bar was
fabricated with cobalt-chrome-molybdenum alloy
(Wironit® BEGO, Bremer Goldschlägerei Wilh,
Germany). The male component of the locator
attachments was then picked up and secured in
the denture with autopolymerizing acrylic resin.
(Fig 1)
A static load of 100 N was applied in the second
molar region, in both vertical and 45-degree
oblique directions, using a universal testing
machine (EMIC-DL 3000, Universal Test System).
Ten tests were done for each group. During each
load sequence, the isochromatic fringes were
observed and photographed within the field of the
circular polariscope with a digital camera (Canon
EOS 1300D) with a resolution of 5,184 x 3,456
pixels, while the prostheses were under load for
one minute. The changes in colored fringe patterns
on load application were clearly captured. The
fringe orders were determined by Tardy method
of compensation. 5 points were considered for
determining the strains;Point 1: mesial-cervical,
Point 2: Mid-mesial, Point 3: Apical, Point 4: Mid-distal, and Point 5: Distal-cervical. (Fig 2)
Stresses in the marked points were determined
using the stress-optic law and from these stress
values, amount of strain in a particular region
was determined. Strain distribution data were
generated for both conventional implants and short
implants under both axial and oblique loading.
The collected data were analyzed by unpaired
t-test (student t-test).
The pattern and distribution of strain were different
under vertical and oblique loading.
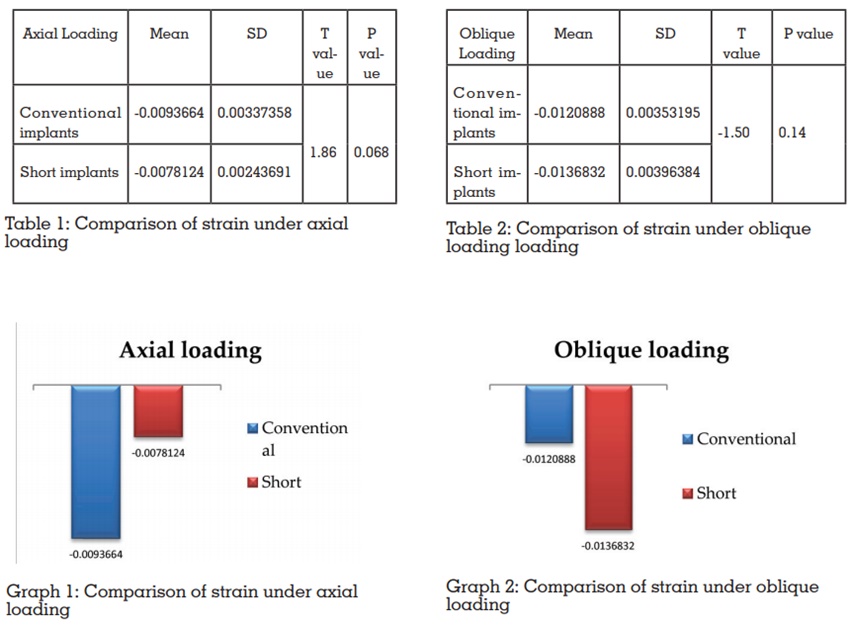
The compressive strains generated by conventional
implants under axial loading was more than short
implants but it was not statistically significant
(p=0.068). A marked increase in strain was noted
in the apical region of conventional implants.
Under oblique loading condition, short implant
generated higher strain than conventional implant
but the difference was not statistically significant.
But a significant increase in strain was noted in the
crestal region of the short implant under oblique
loading. (p=0.14)
The strains generated by conventional and short
implants under oblique loading was significantly
higher (p=0.008, 0.001) than that of axial loading.
In both cases, oblique loading showed greater
strain with higher concentration in the crestal
region.
Implants in conjunction with Kennedy’s class I
RPD was used for the first time in the early 1970s,
and since then clinical trials have indicated good
implant survival rates7
. The response of bone
to applied stress has been well documented to
influence the success or failure of an implant8
.
As far as implant shape is concerned, design
parameters that primarily affect load transfer
characteristics (the stress/strain distributions in the bone) include implant diameter and the length
of the bone-implant interface.
Mandibular posterior region is found to undergo
continuous resorption with time. Previous studies
have correlated this resorption with reduced muscle
activity9
. The main factor to be considered is the
difficulty in finding bone height and thickness
in the posterior region of the mandible sufficient
for placing a conventional implant to support a
prosthesis without the need for lateralization of the
mandibular nerve or bone graft3
. The reason can
be attributed to long-standing edentulous ridges.
Short implants in this region are an interesting
alternative and a therapeutical option to vertical
augmentation since the treatment is faster, cheaper,
and associated with less morbidity5
. Recent studies
have shown positive results for short implants even
for those shorter than 7 mm in length10.
Implants were placed in the second molar region
as many investigations have mentioned that the
location of an implant underneath the denture base
is closer to the second molar, better the occlusal
support11,12.
The overdenture was attached to the implants
using locator abutments on both sides. The
locator attachments are an alternative to ball
attachments, especially when the interarch
distance is inadequate to avoid the denture base
deformation and fracture13. The 100N load selected
represents a load relative to a standard bite force
for a patient with an RPD and was a load that the
photoelastic model could repeatedly withstand
without deforming14,15.
A photoelastic analysis was done to evaluate
the strains. Photoelastic models have been used
successfully to indicate the differences between
various prosthetic designs and the effects of
compromised conditions through a comparative
evaluation of stress-related outcomes6
.
There was no statistically significant difference
between conventional and short implants under axial and oblique loading. The results comply
with the previously published work which has
shown that the behavior of conventional implants
is similar to short implants1,5, 7,10,16,17,18,23. However, a
few studies have shown that a reduction in implant
length increased stress values with a significant
difference3,8,19. This difference could be because
most of the studies were done on fixed prosthesis
and characteristics of implants under removable
prosthesis may be variable.
In conventional implants and short implants, the
strains under oblique loading were more compared
to axial loading which was statistically significant.
Many studies have shown that the nonaxial forces
tend to cause uneven strain distribution leading to
areas of higher strains and others of low strains7
.
This coincides with the findings of Barbier et al
(1998) and non-parametric computerized models
of loaded dental implants by Meijer et al (1996)
and Lai et al (1998)7
. Many clinical studies had
agreed that more bone loss has been observed
around dental implants under oblique loads than
those under axial loads20.
Conventional implants showed higher strain in
the apical region under axial loading. (Fig 3) A
study had compared implant supported distal
extension removable prosthesis with different
attachment types and shown that in the vertical
application of 100 N load in resilient-resilient
attachment type, stress was more in the apical
region (21). In short implants, the strains in the
crestal region were slightly higher compared to
apical but it was not significant.(Fig 4) However,
a study done by Marcele et al have shown that
under axial loading short implants increased stress
concentration around the implant especially in the
cervical portion (23)(Table 1, Graph 1)
Both conventional and short implants showed
maximum strain in the crestal region and
least strain in the apical region under oblique
loading.(Fig 5,6) A study had compared the stress
distribution with different implant dimensions in
implant-supported partial overdentures and has shown that higher stresses around the implant neck
may be attributed to the fact that this area is mainly
subjected to non-axial masticatory forces, which act
in an oblique direction as in grinding movements,
in comparison to the chopping movements, which
act in an axial direction7
(Table 2, Graph 2)
A two-dimensional finite element analysis
suggested that the modulus of elasticity of the
cancellous bone play a key role in good stress
distribution. When a load is applied to the
superstructure, the resultant stress transfers to
the bone surrounding the implant. When there is
a small difference in the values of the modulus
of elasticity of both cortical and cancellous bone,
the stress will be distributed evenly. Since a dense
bone has the ability to bear the stress which is
applied to it, while in the case of great difference,
the stress will be concentrated on the cortical
bone22.
This study had a few limitations too. Photoelasticity
requires the use of special light-polarizing
materials that may not be fully representative
of bone in terms of mechanical behavior10. The
implant osseointegration and the physiological
mobility of the abutment teeth were not considered.
This study only looked at one IARPD design and
did not consider the numerous designs that could
be adopted23. Long-term follow-up clinical studies
are also recommended to assess the results found
in the present in vitro study.
The use of dental implants can be definitely
recommended for treating all edentulous area.
Also, alveolar bone is preserved after dental
implants and a high degree of success is achieved
with implants in partly edentulous jaws24.
Within the limitations of this in vitro study, the following conclusions were drawn: