Cleft lip and palate are common congenital anomalies, with profound aesthetic and functional implications both in the short and long term. The primary concern in infancy is to achieve optimal systemic health of the baby, so that reconstructive surgery can be performed and the cleft segments approximated and molded to facilitate good post surgical aesthetic results. In the present case study, significant objectively assessed improvements were observed in the infant’s feeding, weight gain, approximation of cleft segments, and aesthetic outcome through the proper use of a feeding plate and presurgical naso-alveolar molding (PNAM). Parent cooperation and lactation education were key to treatment success.
Key words: Presurgical nasoalveolar molding; Unilateral cleft lip and palate; Infant orthopedic appliances; Aesthetic outcome; Cleft rehabilitation
Cleft lip and palate are one of the commonest
congenital deformities. They can be found
as a single entity or in the syndromic form.1
Incidence of cleft lip and palate in North India
is approximately 1 in 600 to 800 live births.2
With advancements in technology, prenatal
assessment of clefts is possible, which helps
in formulating treatment plans and mentally
preparing parents for the condition. Literature
suggests that multiple etiological factors, like
genetics, maternal physiological factors, and
smoking, are responsible for cleft lip and palate.3
Problems associated with cleft lip and palate
infants include impaired suckling because of a
lack of negative pressure, due to direct oro-nasal
communication, and affected appearance with
adverse social and psychological implications
for the patient and parents. Slow growth and
development of infants occur due to inadequate
feeding because of factors like excessive air intake during feeding and requirement of a
longer feeding time due to muscle fatigue.4
Regurgitation, aspiration, and upper respiratory
tract infections are well-known risks. The motor
pattern of speech development gets impaired as
proper closure of oro-nasal passage is required
to produce specific sounds. The cleft leads to
disruption in growth and appearance of the mid
facial region, specifically affecting the upper
lip and nose. This requires multiple corrective
surgeries starting from when the individual is a
few months old, and may still produce less than
satisfactory results, if naso-alveolar molding is
not done.
Therefore, treatment is multidisciplinary,
including the Orthodontist, Prosthodontist,
Plastic Surgeon, and Speech Therapist. The
role of the prosthodontist in the management
of cleft lip and palate patients has changed
significantly in the past 40 years.5 Initial naso
alveolar molding by the prosthodontist and
parent education about lactation are the first
steps towards successful long-term treatment of
such cases. Pre-surgical naso-alveolar molding
(PNAM) makes appropriate alterations to the
feeding plate, approximating and optimally
positioning the palatal segments, decreasing
cleft size. Subsequently, the nasal deformity
comprising of depressed columella and/or
meganostril is addressed when the soft tissues
are still plastic and amenable to forces applied
by molding. Absence of molding can lead to
visible scarring and contracture at the cleft site.
Molding leads to a better immediate and post
surgical aesthetic outcome, apart from obvious
improvement in systemic parameters due to
obturation of the communication by the feeding
plate. Such appliances cannot be successful
without the cooperation and understanding of
parents. Further, counseling parents regarding
feeding is of utmost importance in managing
such cases. A case study harmonizing the above factors leading to a successful outcome
is described.6
A 10-day-old patient with a congenital right
unilateral complete cleft involving the lip,
alveolus, and hard as well as soft palate, was
referred from the Department of Pediatrics
for fabrication of a feeding plate. Because of
insufficient feed, the baby was weak and had
poor growth. At the time of birth, the weight of
the newborn was 3.10 kg, which decreased in the
first week to 2.50 kg.

An initial examination revealed a Veau’s class III
defect (Figure 1a, 1b). Primary impression was
made using addition silicone putty (Zhermack
Hydro Ride, Italy), with the infant lying in face
down position and patency of airway ensured by
the infant crying. Impression was evaluated, and
cast poured in dental stone (Kalstone, Kalabhai
Karson Pvt Ltd, India). After blocking undercuts
on the cast and providing the missing palatal
and alveolar segments with proper contour
using modelling wax, a feeding appliance was
fabricated using autopolymerizing polymethyl
methacrylate (DPI cold cure, Mumbai). The
posterior extension of the feeding plate was
ensured visually and by the absence of gag
stimulation. Intaglio surface of the feeding
appliance was finished and polished to avoid
abrading the delicate mucosa, ensuring that it
did not extend into the palatal or alveolar defect,
to facilitate gradual approximation of the palatal
segments. The posterior margin of the feeding
plate was kept paper-thin. A small mushroom
shaped retentive button of clear acrylic resin
was made on the feeding plate, in the centre of
the alveolar cleft site, at a 45-degree outward
angle to the occlusal plane. This was to ensure
that the button did not interfere with the lip seal
during suckling.
Two elastics of 3/16” (Dentosmile Orthodontic Intraoral Latex Elastics, India), were wound on
the button with medical tapes (0.25 inches wide,
Transpore tape, 3M India Limited), extended
slightly upward and laterally, and attached to
Base Tapes (0.5-1.5 inches wide, Micropore,
3M India Limited) which were stuck on the
cheek, about a finger width below the eye. This
mechanism helped retain the feeding plate and
provide anchorage for subsequent naso-alveolar
molding. Proper suckling with no gagging and
training of parents in positioning the plate
were ensured before delivering the prosthesis.
Medical tape extending between the nasolabial
lines to approximate the cleft lip segments
from the first appointment helped bring the lip
segments together.
Parents were informed about the importance
of feeding in helping the baby reach adequate
parameters for the lip surgery. They were
instructed to use a milk bottle with milliliter
markings and a soft, long nipple, to record the
amount of milk consumed, to monitor the ease
or difficulty of suckling, and to keep the baby in
a semi-reclining position while feeding to help
direct the milk posteriorly toward the oropharynx
without regurgitation. Such instructions, with
regular reminders, become even more crucial in a
context where the parents are socio-economically
or educationally disadvantaged. Weekly follow
ups included weight measurements to assess
growth and cleft space measurements on a cast
to evaluate appliance efficacy.
Alveolar molding was initiated one week after
delivering the feeding plate, ensuring the baby
was comfortable and the caretaker was inserting
the appliance properly. One millimeter of silicone
based relining material (Detax mollosil soft liner,
DETAX GmbH, Ettlingen, Germany) was added
to the feeding plate in areas where the alveolar
segments needed to be directed away, and a
corresponding 1 mm of acrylic was removed from
the plate in regions where the alveolar segments
needed to move into position. The goal was to
move the larger alveolar segment inward and toward the smaller segment, and to move the
smaller segment outward (anteriorly) and toward
the larger segment until they approximated each
other and were in a better position for surgical
union. Therefore, these sequential additions and
removals were performed weekly.
After the gap between the alveolar segments was
reduced to about 6mm, a swan’s neck shaped
nasal stent was bent from a 19-gauge stainless
steel wrought wire, with one end inserted into the
feeding plate near the retentive button, and the other end passively contacting the centre of the
mucosal aspect of the affected ala. The shape of
the wire ensured enough clearance from the cleft
segment for lip taping, and an outward force on
the ala when activated. The tip of the stent was
covered with an inner layer of autopolymerizing
polymethyl methacrylate and an outer layer
of soft liner, in the shape of a small bead. The
nasal stent was activated outward and forward
to produce a slight blanching of the ala. The
purpose was to pull the deviated bridge of the
nose towards the middle of the face and to add
contour to the flattened ala (Figures 1c, 1d).
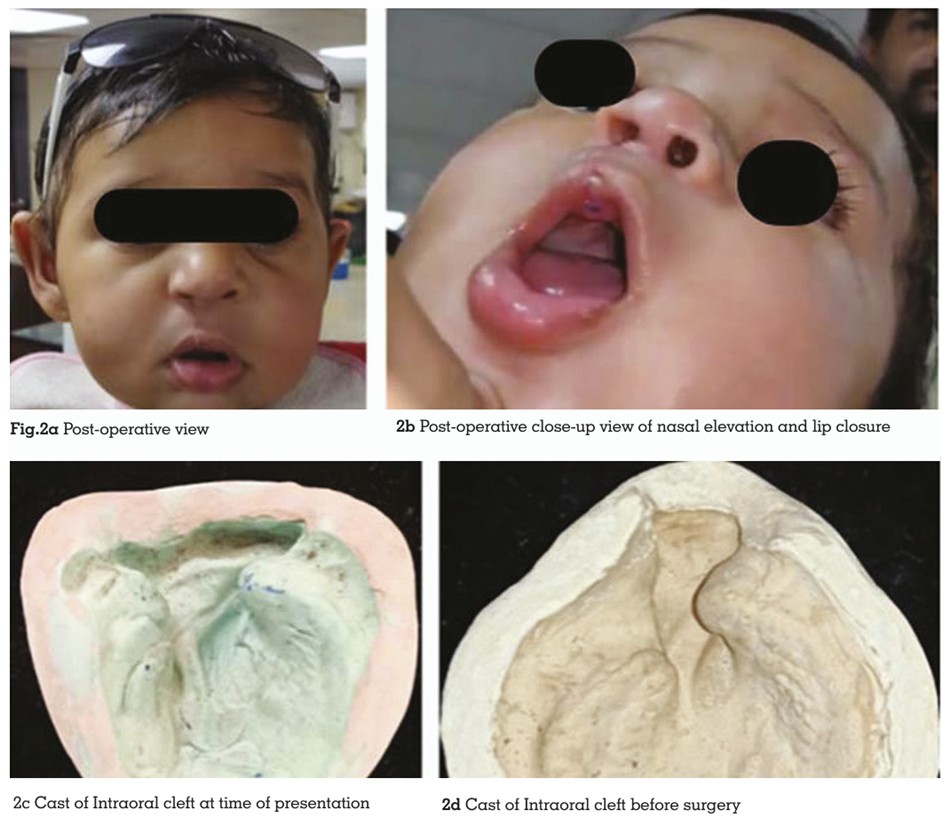
Nasal and alveolar molding was continued at
7–10-day intervals till the infant turned 20 weeks
old (Figure 1e, 1f). By then, positive changes in
the affected oral and facial region and systemic
parameters had taken place (Tables 1,2). Lip
surgery was performed when the infant was 5
months old, with a satisfactory outcome (Figures 2a,2b,2c,2d). The baby was in constant follow
up and observation till writing this report, as the
role of multiple specialties is important for long
term functional and aesthetic success.
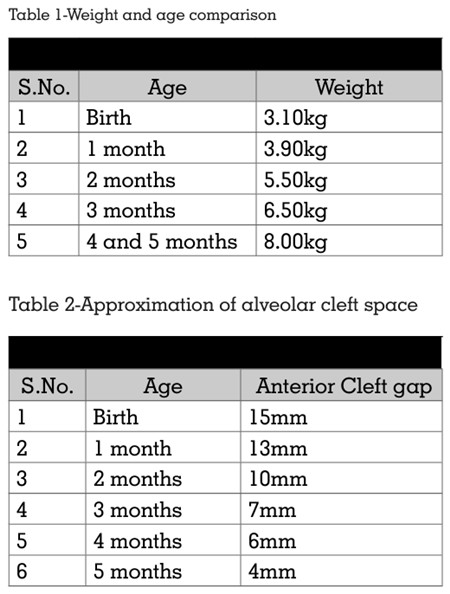
The results with PNAM therapy in this non
syndromic unilateral cleft lip and palate case
were highly encouraging. A notable reduction
in the alveolar cleft width from 14 mm to 4 mm
was observed, along with a visible improvement
in nasal symmetry and contour over a period
of 5 months. These improvements support the
effectiveness of PNAM as an essential pre
surgical adjunct in cleft care. Two critical
factors that contributed to this success were
early initiation of therapy and active parental
cooperation.1,2
Early initiation of PNAM therapy is widely
regarded as pivotal to its success. Newborn
tissues are more moldable due to the elevated
levels of maternal estrogen, which increase
hyaluronic acid in the cartilage and connective
tissues. This window of plasticity offers the best
opportunity to reshape the nasal cartilage,
align alveolar segments, and support optimal
soft tissue adaptation. Delayed initiation, on
the other hand, may result in reduced tissue
responsiveness, making it more difficult to
achieve desired aesthetic and functional results.
It can also prolong the total treatment time
and may necessitate more extensive surgical
intervention later.7
Parental involvement cannot be overemphasised
in PNAM therapy. The parents are responsible
for correctly placing the appliance multiple
times a day, maintaining hygiene, monitoring
feeding and growth, and ensuring timely
follow-up appointments. These responsibilities
are more efficiently managed by literate and
motivated caregivers who understand the nature
and goals of the treatment. At our center, we have observed a direct correlation between
parental awareness and treatment success.
Providing comprehensive training to parents—
including how to place lip taping, secure the
appliance, feed in upright positions, and track
weekly weight gain—has proven beneficial.
Moreover, parental education plays a larger
societal role in reducing the stigma surrounding
cleft conditions by spreading awareness and
improving community acceptance.8
Despite the advantages, PNAM therapy is not
without its complications. The most common
include tissue ulceration due to pressure from the
appliance or faulty placement/ removal, irritation
from taping, and poor appliance retention. These
can usually be managed through timely recall
examinations, use of biocompatible soft liners,
and reinforcing instructions to the caregiver. A
dedicated and trained team monitoring these
factors significantly reduces adverse effects.
The “Rule of 10s” is a widely accepted surgical
guideline that recommends cleft lip repair be
undertaken when the child is at least 10 weeks
old, weighs 10 pounds (approximately 4.5 kg),
and has a hemoglobin level of 10 g/dL. PNAM
therapy is ideally completed before this timeline,
aligning with these criteria and optimizing
surgical outcomes.9
There exists a divergent school of thought that
questions the significance of PNAM. Critics argue
that the effects of PNAM may be short-term and
that nasal morphology can relapse post-surgery
without continued nasal support. Some studies
also suggest that surgical techniques alone
may yield comparable results in experienced
hands. However, proponents counter that
PNAM minimizes tissue tension during surgery,
improves surgical precision, and reduces the
need for extensive nasal revision later.6,7,11
It has been stated that educating parents
about causative factors, the significance of management, and follow-up of the condition
during the prenatal period often reduces
parental anxiety or depression and motivates
them to seek early treatment. It also improves
the psychological and cosmetic outcome for
patients.10,11 Patel et al concluded that pre
surgical nasoalveolar molding helped reduce
the cleft gap, improve arch form, approximate
lip segments, and distinctly improve the nose
morphology by correcting flattened nasal wings.6
At the conclusion of PNAM therapy, primary
cheiloplasty (cleft lip repair) is the standard
surgical procedure undertaken. Depending on
the case and surgeon’s preference, techniques
like Millard’s rotation advancement or Tennison
Randall’s triangular flap method may be
employed. The goals are to achieve proper
muscular continuity, symmetrical nasal and lip
contours, and a favorable long-term aesthetic
outcome. The groundwork laid by PNAM in
approximating the segments and improving
nasal symmetry significantly contributes to the
success of this surgery.2,3,6,7
Early institution of treatment, regular recalls
for molding, weekly cleft dimension and weight
measurements, and parental counseling,
education, and compliance are extremely
important in improving the prognosis of PNAM
in cleft lip and palate babies. PNAM therapy
remains a cornerstone in modern cleft care,
especially when initiated early and supported
by well-informed, cooperative caregivers. Its
multifactorial benefits—ranging from surgical
ease to societal integration—underscore its
relevance in both clinical and psychosocial
domains.