Dental implants have been a broadly recognised treatment modality to replace missing teeth and in order to restore the oral functions. The utilisation of root form endosseous implants have increased considerably and this option has become much more sophisticated with the introduction of latest designs and concepts. Long term post placement studies have revealed that prosthetic complications, including screw loosening, screw fracture, framework and implant fracture. Abutment screw loosening is the second most cause of failure of implant supported crowns, after loss of osseointegration. This condition is mostly witnessed in single implant supported restoration. Management of screw loosening is a challenging procedure and this clinical report describes the management of an implant abutment screw loosening of lower back teeth region with minimal damage to the existing restoration making it possible to be reused.
Key words: Dental Implant, Implant Abutment Screw loosening, pre load, splinted cement retained implant prosthesis
The replacement of missing teeth by implant
supported prosthesis has become a popular
option after the introduction of the concept of osseointegration with titanium fixtures1,2. The use
of root form endosseous implant has increased
considerably and this restorative option has
become more refined with the introduction of
newer designs and concepts. Screw loosening,
screw fracture, prosthetic component and implant
fractures are the different prosthetic complications
seen after loading the implant3–5. Among these,
screw loosening is the most common complication.
This is seen more in single implant supported
prosthesis with external connection and molars6–9.
Reasons for screw loosening include inadequate
preload, inappropriate implant position and
occlusal scheme, variations in hex dimension
and abutment counterparts, differences in fit and
accuracy, tension on abutment, improper screw
design and excessive occlusal forces10–12.
A 45 year old female patient reported to The MAHE
Dental College, Department of Prosthodontics with
a chief complaint of dislodged implant crown and
misfit implant crown in the right lower back tooth
region. (Fig. 1)
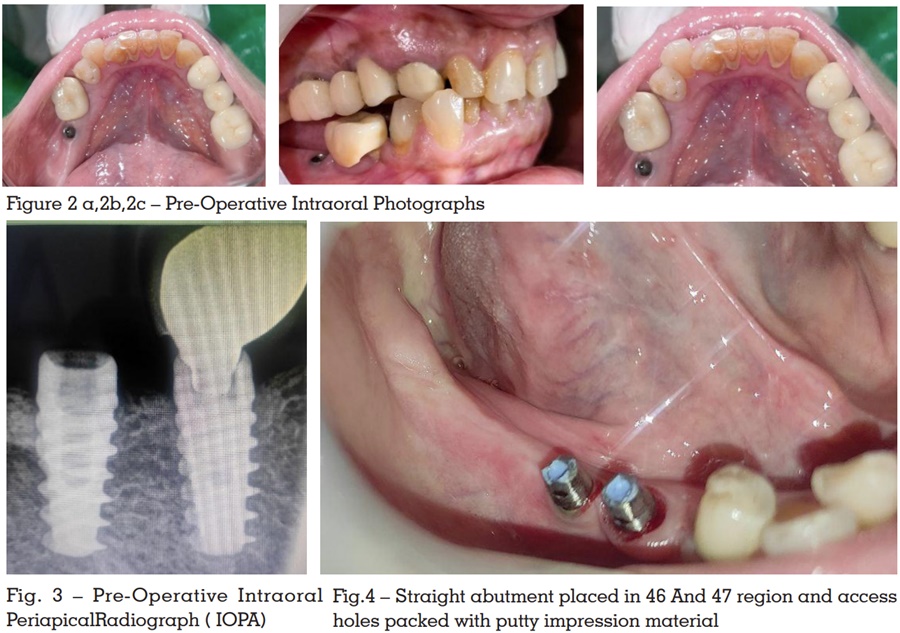
On examination, implant crown in 47 was dislodged
and the implant crown in 46 was rotated. RVG
was made and the radiographical assessment revealed discrepancy between the transmucosal
abutments and the fixture head which indicated
implant abutment screw loosening in 46 and
dislodged crown in 47 (Fig. 2a,2b,2c). Both the
implant prosthesis were screw retained. (Fig. 3)
As the loose crown was causing discomfort to
the patient, it was sectioned and the screw and
abutment were retrieved. 46 and 47 were done
under paltop implant system.
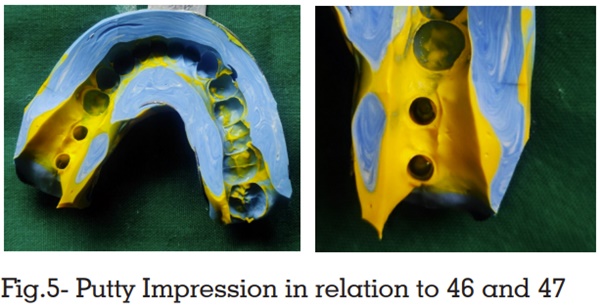
Suitable straight abutment were screwed and
adequate preparation was done. After acquiring
adequate clearance, the access holes were packed
with putty impression material and an abutment
level impression were made using addition silicone
and light body for fabricating a splinted cement retained implant prosthesis in 46 and 47. (Fig.4,
Fig.5)
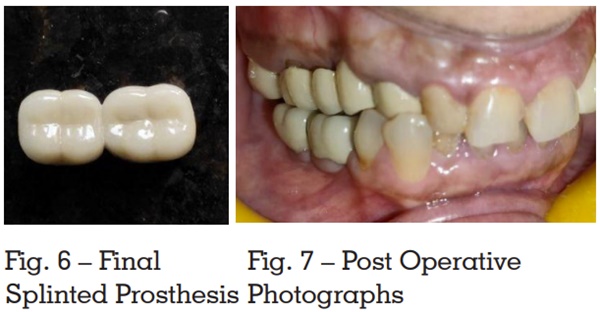
Prior to cementation, the access holes were packed
with putty impression material and GIC. The
splinted PFM implant prosthesis was luted with
GIC (Fig.6, Fig.7). Excess cement in the proximal
aspects were flossed.
This case report illustrates one of the mechanical
complication which can occur during prosthetic
stage of implant surgery. The radiovisiography
revealed discrepancy between the transmucosal
abutments and the fixture head which indicated
implant abutment screw loosening in 46 and
dislodged crown in 47. The reason for screw
loosening was due to inadequate application
of tightening torque to generate the necessary
preload. The screw loosening of implant abutment
can cause issue for both the dentist and patient .It
is essential to sacrifice the overlying restoration
to give access to the screw. Screws have been
studied considerably in the engineering literature
and dental implant screws have been improved
as a result.
Proper design of the occlusion and sound
osseointegration, a reliable connection between
implant and abutment is important for the
appropriate functioning and stability of implant
restoration. Several clinical studies have reported
incidences of abutment loosening in various types of abutment connections. The external hex
configurations is more prone to abutment screw
loosening. Limited engagement of the external
member and the presence of a short fulcrum point
when tipping forces are acting, are the main reason
for abutment screw loosening in external hex
connections. In the external hex configuration, the
axial preload of the abutment screw determines the
stability of the connection. There is no lock form or
positive locking by the external hex. The rotational
position was determined by external hex but it does
not absorb any lateral loading and the tensile force
and so the stress is concentrated on the abutment
screw. Different methods have been tried to reduce
the screw loosening. The two important methods
used to counteract screw loosening include the
incorporation of an antirotational element and
attaining optimum screw joint preload.
Several guidelines recommended for improving
screw joint stability include centering the occlusal
contact, flattening the cuspal inclination, proper
tightening of the abutment screw, narrowing the
buccolingual width of the restoration, and reducing
cantilevers. Incorporation of these features into
the restoration will help to decrease the incidence
of abutment screw loosening. There are three
methods for managing abutment screw loosening.
The most conservative method is removal of the
crown along with the abutment as described in
the case report. The second method is to identify
the access of the connecting screw head. The
access may be labial, occlusal or lingual. This
should be identified during the cementation of the prosthesis. The abutment connecting screw is then
removed or re-tightened through the perforation
made at the access in the crown. Depending on
the location of the access the crown, it can be
reused or discarded. The third method include
vertical cuts made on the crown to separate the
crown from the abutment.
A conventional mode of managing abutment
screw loosening without consecrating the crown on
various reasons for abutment screw loosening has
been described. Inadequate preload is the most
accepted reason for abutment screw loosening
in two piece endosseous root form implants.
Employing suitable tightening torque with wrench
having torque gauge will deliver the optimum
preload and splinted crowns can be utilized for
such clinical situations.