A child born with cleft lip and palate may experience difficulties while feeding. It is the most common congenital craniofacial malformations. Feeding difficulties should be assessed and intervened as early as possible, as they are an important aspect of the multidisciplinary team approach in the management of cleft lip and palate. Feeding obturators improve feeding thereby contributing to weight gain and a thriving state of health, a prerequisite for surgical repair of the defects. A successful prosthesis should meet the physiological, psychological and aesthetic needs of the patient. This article describes the procedure for rehabilitation of cleft palate patient with feeding plate.
Key words: Feeding plate, cleft lip and palate, Neonate.
Cleft lip and palate (CLP) is one of the most
common congenital craniofacial defects. Cleft
palate (CP) is a fissure in the midline of the palate due to failure of the two sides to fuse
in embryonic development1. Its consequences
affect several system and functions that includes
feeding, dentition, speech as well as the social
and psychological problems which have an impact
on the child and the parent.2
Neonates born
with cleft palate have oronasal communication
which diminishes the ability to create negative
pressure necessary for suckling.3
The feeding plate
obturates the cleft and restores the separation
between oral and nasal cavities. It creates a rigid
platform towards which the baby can press the
nipple and extract the milk.4
It facilitates feeding,
reduces nasal regurgitation, reduces the incidence
of choking and shortens the length of time required
for feeding3
. The obturator also prevents the tongue
from entering the defect5
and interfering with the
spontaneous growth of palatal shelves towards
the midline. It also helps to position the tongue
in correct position to perform its functional role in
the development of jaws and contributes to speech
development. The obturator reduces the passage
of food into the naso-pharynx thus reducing the
incidence of otitis media and naso-pharynhgeal
infections.4
Feeding plate restores the basic functions of mastication, deglutition and speech
production until the cleft lip and/or palate can be
surgically corrected.
A 3 days old neonate was referred to the Department
of Prosthodontics with chief complaint of difficulty
in feeding. On examination, it was found that
the child was born with unilateral cleft palate.
Intraoral examination revealed a cleft in the soft
palate and uvula (fig. 1)
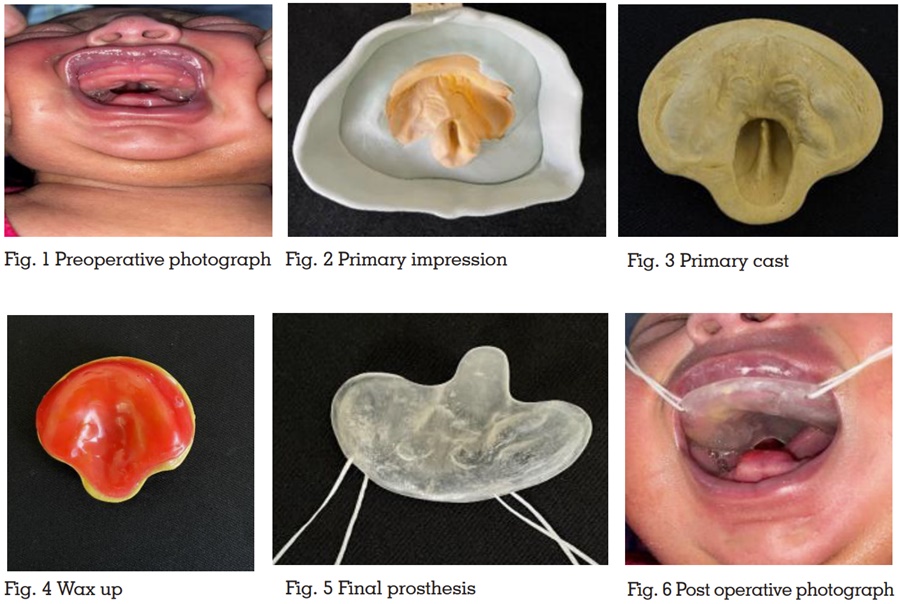
A perforated wooden spoon was selected and
Primary impression of the maxillary arch with the
cleft was made with putty addition silicone. The
wooden spoon was used to carry the impression
material into the infant’s mouth. The polyvinyl
siloxane material was gently pressed against the hard palate and into the buccal and labial
vestibules, while the baby was held in mother’s
lap. The impression was inspected thoroughly (fig.
2). Beading and boxing were done and cast was
poured with type III dental stone with addition of
2% NaCl to decrease setting time (fig. 3). A 2mm
modelling wax was adapted to the cast to form
the feeding plate (fig.4). Flasking, dewaxing and
acrylization was done in conventional manner
with a short curing cycle to lesser the laboratory
time. Heat cured clear acrylic resin was used for
fabrication of feeding plate. After finishing and
polishing, two holes were placed in the anterior
part of the feeding plate and dental floss was tied
for fastening and easy removal (fig. 5). Feeding
plate was checked in patient’s mouth and mother
was asked to feed the baby and check for the
comfort of the same. Post insertion instructions
were provided on how to use and maintain the
feeding appliances (fig. 6).
The main objective during the first month of cleft
palate infant’s life is proper weight gain, which
results from proper feeding, making the infant
ready for future surgical correction.6
Construction
of a feeding plate not only fills the gap between
the nasal and oral cavities, but it also achieves
maximum treatment benefits for such patients;
at the same time it increases awareness and
enhances the skills of diagnosis and management
aspects of all the specialists in the interdisciplinary
team7
.
Making an impression is the first challenging
clinical step in cleft palate infants. The various
factors are lack of cooperation on behalf of
parent, oral cavity is too small to be adequate for
commercially available impression material and
undercuts of the defects.8
Therefore, it is important
to take care of infant positioning, tray used and the
impression material in order to maintain airway
patency during impression making. Prone position
was essential in keeping the tongue in forward
position and avoiding posterior regurgitation of the
impression material. Infant crying was satisfactory
for ensuring airway patency and elimination of
any possibilities of impression material aspiration.
Impression was made with putty because high
viscosity material reduces the aspiration risk.
In addition, it reproduces the areas of interest
reasonably well.
Inadequate nourishment due to difficulty in feeding
affects the health and act as a stumbling block in the milestone of normal development. The
feeding plate overcomes the hinderance which
occur during the normal growth and development
of a cleft patient and thus it should be advised as
early as possible soon after birth. It is a handy,
risk free procedure that can be carried out in the
regular OP and that decreases the stress on the
parents and is a comforting for the infant. It act
as an important tool for feeding, development of
palatal shelves, prevention of tongue distortion,
and nasal regurgitation.