Amelogenesis imperfecta is a hereditary disorder displaying a group of conditions which cause developmental alterations in the structure of enamel. The adverse effects it has on the oral health and quality of life of the individual warrants the identification of the contributing factors for the excessive wear and loss of vertical dimension. Extensive restorative treatment is imperative for the correction of such severely worn out dentition. Rehabilitation in such patients improves aesthetics, function and comfort. This case report presents a systematic approach in rehabilitating a case of hypomaturation type Amelogenesis Imperfecta (AI) following Hobo twin stage philosophy. Keywords: Full mouth rehabilitation, Amelogenesis imperfecta, Hobo’s technique, Hobo’s philosophy.
Amelogenesis imperfect (AI) is a group of inherent
disease that exhibit quantitative or qualitative
enamel defect in the absence of systemic
complication.1
AI represents a group of conditions,
genomic in origin, which affect the structure and
clinical appearance of the enamel of all or nearly all the teeth in a more or less equal manner, and
which may be associated with morphologic or
biochemical changes elsewhere in the body.
Hereditary brown enamel, hereditary enamel
dysplasia, hereditary brown opalescent teeth are
the other terminologies used for AI. The prevalence
varies from 1:700 to 1:14000, according to
population studies.2
AI affects the entire ectodermal
component. Amelogenesis Imperfecta trait can be
either autosomal dominant, autosomal recessive
or X- linked mode of inheritance.3
AI affects both
the primary and permanent dentitions. In the teeth
affected by AI, the dentin and roots appear normal.
Depending upon enamel appearance, structural
and developmental defects, AI is classified
into 4 patterns: hypoplastic, hypomaturation,
hypocalcified, and hypomaturation-hypoplastic.
Hypoplastic form is characterized by the
reduction in enamel matrix thickness with normal
mineralization. Enamel has reduced thickness,
appears normal and is less prone to attrition. The
color appears normal with translucency of a yellow
to dark brown color depending on the thickness of
enamel and dentin.4
Hypomaturation form shows
defect in the mineralization process with normal
matrix formation. Enamel has normal thickness, but hypomineralized and is prone to attrition. The
color may be affected by staining from the oral
environment. Teeth has a mottled appearance
of yellow-brown or red-brown discoloration.4
Hypocalcified form is characterized by defect
in the quality of the mineralization process with
normal quantity of matrix formation. Enamel
has normal thickness with loss of translucency,
hypomineralized, exhibits a soft cheesy consistency
and easily breaks down. Color may be affected
by staining from the oral environment and teeth
appears dark.4
In hypomaturation-hypoplastic
cases, the enamel thickness is drastically
reduced. The crowns show pitting and tend to
have hypomineralized areas.4
This clinical report describes the prosthetic
rehabilitation of a case of amelogenesis imperfecta
following the Hobo twin stage philosophy. Following
a thorough clinical and radiological examination, a diagnosis of hypomaturation type of AI was made.
A 43 year old women reported to the Department
of Prosthodontics, Government Dental College,
Thiruvananthapuram with the chief complaint
of yellowish teeth and bilaterally missing lower
back teeth. Extra oral examination revealed
reduced lower facial height and absence of any
symptoms of temporomandibular disorders due to
the collapsed bite. Intra oral examination revealed
presence of deciduous canines in the maxillary
arch, missing 15, 13, 23, 37, 36, 33, 46 and 47,
caries in relation to 14, 24, 25, discoloured 41,
increased overbite, and most of the posterior teeth
showed early stages of attrition (Figure 1).
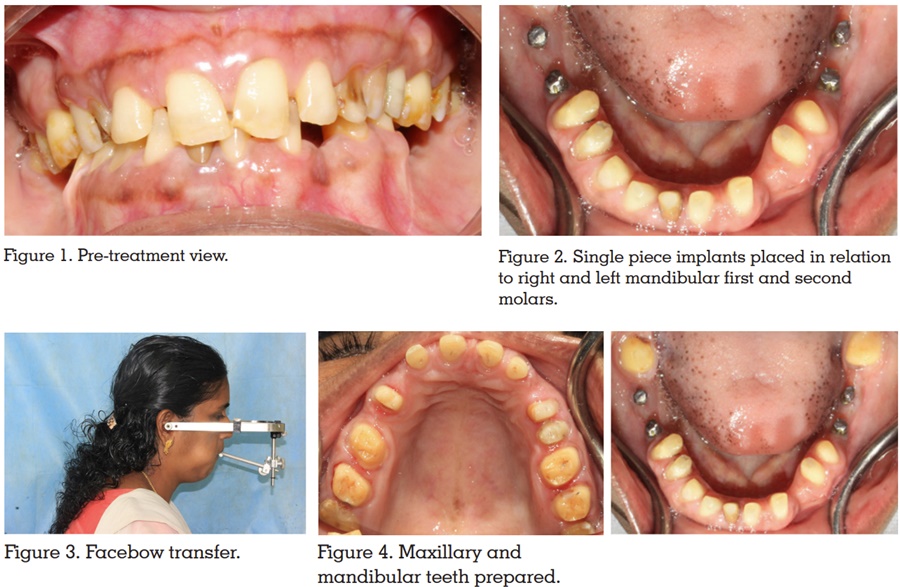
Root canal treatment was indicated for 14, 24, 25 and the maxillary deciduous canines were
extracted. Single piece implants were placed to
replace the missing right and left mandibular first
and second molars (Figure 2). Hobo twin stage
philosophy was opted to rehabilitate this patient
following the osseointegration of the implants.
Diagnostic casts were fabricated and the anterior
segment of the maxillary cast was sectioned as
a single unit from canine to canine and attached
with dowel pins to facilitate the removal of this
part during the wax up of the posterior teeth. A
facebow transfer was done (Figure 3).
The centric relation was recorded using aluwax
and the casts were mounted in a semi adjustable
articulator using the facebow transfer and the
centric relation record. The vertical dimension
of occlusion had to be increased by 4 mm. The
incisal pin was adjusted to fabricate an occlusal
splint of 4 mm thickness and it was then delivered
to the patient. The patient was instructed to wear
the splint for 12 weeks. At the end of twelve weeks,
the patient had no pain in the temporomandibular
joint and she could well tolerate the increased
vertical dimension.
The diagnostic wax up was completed which
helped the patient to visualize the final outcome
of the treatment and also aided in the fabrication of
temporary crowns to be cemented after the crown
preparation. The diagnostic wax up was fabricated
following condition 1 for posterior teeth wax up and condition 2 for anterior teeth wax up. A lucia jig
was made on the maxillary central incisors such
that the vertical dimension was increased by 4 mm.
Maxillary and mandibular posterior teeth were
prepared first and the inter-occlusal clearance was
confirmed by placing the lucia jig on the anterior
teeth. Temporary crowns were fabricated and
positioned on the posterior teeth and these crowns
helps to determine the interincisal clearance while
preparing the anterior teeth. Following this, the
maxillary and mandibular anterior teeth were
prepared (Figure 4).
The posterior temporary crowns were removed,
gingival retraction was done and a two stage putty
and light body impression was made for both the
arches. Temporary crowns were then cemented
with zinc oxide eugenol cement. Metal copings
were fabricated for the anterior as well as posterior
teeth and try in was done (Figure 5).
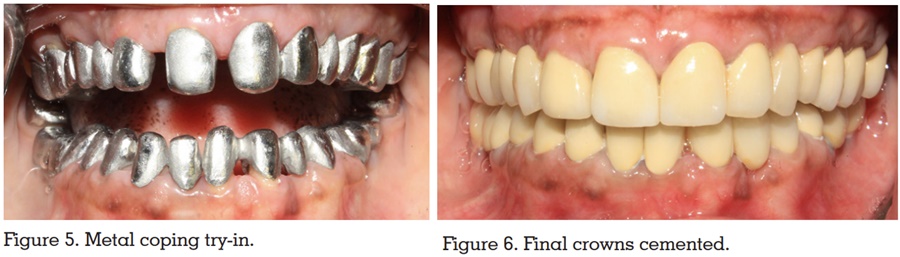
A centric relation record was made with the metal
copings in situ. During the phase of ceramic
layering, the articulator was set to condition 1,
maxillary anterior segment was removed and
ceramic layering of the posterior teeth was done
followed by ceramic layering of anterior teeth when
the articulator was set to condition 2 and maxillary
anterior segment re-attached. A group function
occlusion was achieved after the final contouring
and adjustment. A bisque trial was carried out
where necessary adjustments were done. Following
this, the final restoration was cemented with glass ionomer cement (Figure 6). The patient was
recalled for routine examination at one, three and
six months after the final cementation. She was
satisfied with her appearance and functional
improvements as well. She exhibited no signs of
TMJ pain.
Early gnathological concepts focused primarily
on the condylar path as it was theorized to be
a constant through adulthood. McCollum and
Stuart concluded from a study conducted on 10
patients that condylar guidance is dependent on
the anterior guidance.5
Anterior guidance was
considered to be at the discretion of the dentist.
In prosthodontics, the condylar path has been
considered the main determinant of occlusion.
According to the twin-table technique by Hobo,
the cusp shape factor and the angle of hinge
rotation are derived from the condylar path.5
These
factors contribute to the determination of an ideal
anterior guidance. However, in the twin-stage
procedure, the cusp angle was considered as the
most reliable determinant of occlusion. This was
according to the proven data from studies that
the cusp angle was four times more reliable than
condylar and incisal paths.6
In the twin-stage
procedure, to provide disocclusion, the cusp angle
should be shallower than the condylar path. To
make a shallower cusp angle in a prosthesis, it
is important to wax the occlusal morphology to
produce balanced occlusion or articulation so that
the cusp angle becomes parallel to the cusp path
of opposing teeth during eccentric movements.7
Since anterior teeth help to produce disocclusion,
the anterior portion of the working cast becomes an
obstacle. Also, when fabricating the anterior teeth
to produce disocclusion, some guidance should
be incorporated. In this conditional approach
described by Hobo, a cast with a removable
anterior segment is fabricated. Reproduction of
the occlusal morphology of the posterior teeth is
done without the anterior segment and a cusp angle coincident with the standard values of
effective cusp angle is produced (referred to as
“condition 1”).8
Second, reproduction of the anterior
morphology with the anterior segment is done and
anterior guidance which produces a standard
amount of disocclusion is provided (referred to
as “condition 2”).8
Measurement of the condylar path is not
necessary in hobo twin stage philosophy, hence
complicated instruments such as the pantograph
and fully adjustable articulator are not required.
Therefore, this procedure is much simpler than
the standard gnathological procedure, yet it
follows gnathological principles. This technique
is suitable for restorative work for patients with
temporomandibular disorders and splint therapy
as the condylar path is not considered as the main
determinant of occlusion. This procedure can also
be incorporated easily with commonly used clinical
techniques such as face-bow transfer, various
centric recording methods, and the cusp-fossa
waxing. The contraindications of this technique
are abnormal curve of Spee, abnormal curve of
Wilson, abnormally rotated teeth, and abnormally
inclined teeth.
The principles and concepts involved in oral
rehabilitation using the Hobo twin-stage procedure
have been discussed. The amount of disclusion
of teeth is significantly controlled by the condylar
and incisal guidance and disregards the role
of measured condylar guidance. The average
calibrations of condylar, lateral and incisal
guidance and cusp angle provide an easy
approach of management with lesser skills needed.