Edentulism is a commonly occurring condition in elderly and rehabilitation becomes pertinent to restore the lost function. Single stage surgical protocols with immediate restoration of function has emerged as an effective treatment approach over the past years. All-on-4 approach, avoids the complicated procedures of bone grafting and ridge augmentation and delivers immediate restoration. A fully guided all-on-4 surgery minimizes the risks and errors involved with free hand surgery especially in the maxillary arch, and provides a more controlled approach with predictable outcomes. A combination of 3D planning and surgical template, the all-on-4 protocol, and immediate functional loading is used in this case report.
Key words: All-on-4 concepts, Fully guided surgery, Radiographic template, Dental implant, Edentulism, Immediate prosthetic rehabilitation.
Loss of teeth can have a negative functional as
well as psychological impact on an individual. This loss can be the consequence of various factors
such as caries, improper oral hygiene further
leading to periodontal diseases. Edentulism has
been shown to have an adverse effect on quality
of life as well as overall health of the patient.1
Various treatment modalities have been used
to rehabilitate the edentulous arches aiming
at restoring the functional efficacy as well as
esthetics of the patient. Conventional complete
dentures have been a routinely done treatment
option from way back. However, poor stability,
compromised retention, reduced oral sensory
function and problems associated with denture
care and handling are a few of the reasons
for patient dissatisfaction.2
Also, the mental
satisfaction of a fixed prosthesis is what draws
the patients towards implant supported prosthesis
over a conventional removable denture. An
osseointegrated implant supported fixed prosthesis
makes the final treatment result more predictable
and acceptable to the patient. Immediate loading
of implants have emerged as a reliable treatment
approach with high success rates and more
predictable outcomes over long term follow ups.3,4
Immediate rehabilitation enhances the end result
with appreciable esthetics, phonetics as well as functional productivity, making the final prosthesis
more admissible.5,6
Rehabilitation of atrophic edentulous arches with
implant supported prosthesis is a prosthetically
complex situation and often involve placement
of tilted implants based on the availability of
bone for achieving osseointegration as well as
the resultant optimum implant stability. Various
anatomic factors such as proximity to the
inferior alveolar nerve in the mandibular arch
and excessively pneuamatized maxillary sinus
can pose a hindrance to the traditional implant
placement. All-on-4 concept first came into light
from the concept of Malo et al. and has evolved
over time. It presently utilizes a combination of
2 straight anterior and 2 tilted posterior implants,
hence providing enough support to maintain a
full-arch fixed prosthesis. Angulation of distal
implants provides numerous biomechanical and
clinical advantages for fixed restorations with less
invasive techniques when compared with grafted procedures with traditional axial implants.7
A
fully guided surgery making use of a customized
surgical template ensures an accurate diagnosis
and treatment planning followed by a precise
implant placement enhancing the accuracy of the
final prosthesis. In this case report, we describe a
controlled approach of rehabilitating edentulous
arches with fully guided all-on-4 implant surgical
protocol followed by immediate provisionalization.
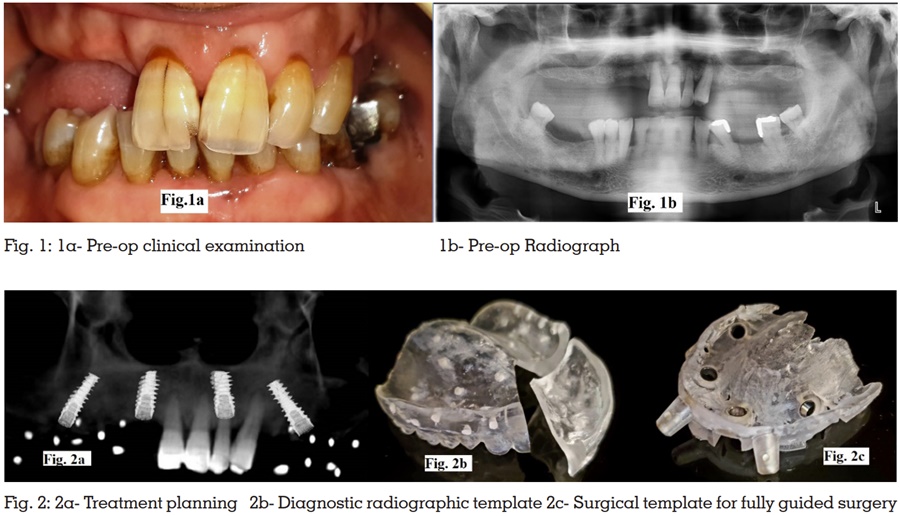
A 60 year old male reported to the Department
of Prosthodontics with the complaint of difficulty
in mastication due to missing teeth in maxillary
posterior region. On intraoral examination, 11,
21, 22 and 23 were present in the maxillary arch
(Fig.1a) and the teeth were Grade 2 mobile.
Teeth number 34, 36, 46 and 47 were missing in
the mandibular arch. Radiological examination
revealed the vertical as well as horizontal bone loss
around the maxillary teeth (Fig.1b). Considering the amount of bone loss and mobility associated, the
patient’s inclination towards a fixed prosthesis and
declination for an invasive surgery, extraction of the
remaining maxillary teeth was planned followed
by rehabilitation with all-on-4 technique. According
to Bedrossian classification,8 our case fell into
the category where in bone is present in Zone I
and Zone II only guiding us to a prosthetic option
of rehabilitating the anterior maxillary region
with traditional implant placement and posterior
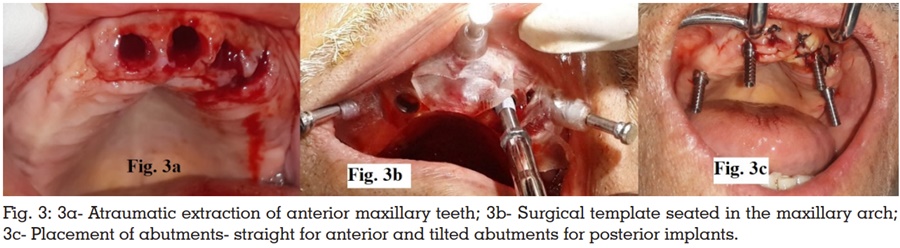
maxillary region with tilted implants. Hence, an
All-on-4 approach of rehabilitation was planned
for the maxillary arch (Fig.2a) and conventional
implant placement was planned for replacing
the missing teeth in the mandibular arch. A fully
guided All-on-4 surgery was planned using Nobel
Guide. Firstly, a diagnostic radiographic template
was fabricated (Fig.2b) to assist in acquisition of
radiographic scans required for planning the final
implant positioning and further for the fabrication
of a fully guided surgical template to be used
during the surgical procedure. For the fabrication of the radiographic template, a preliminary
impression of the maxillary arch was made using
irreversible hydrocolloid and stone model was
poured. A tentative jaw relation of the patient was
recorded and the maxillary and mandibular casts
were articulated using this relation. Following this,
a transparent complete denture was fabricated for
the maxillary arch keeping in mind the esthetics,
phonetics and occlusion with respect to mandibular
arch. This transparent denture was to serve as
the diagnostic stent. This stent was sectioned in
two parts, one anterior part corresponding to the
anterior maxillary teeth present in the patient’s
mouth and one posterior part for the posterior
edentulous maxillary arch. Radiopaque markers
were incorporated within the diagnostic stent
corresponding to the final implant position required
for the procedure. The posterior section of the
stent was seated in the patient’s mouth and 3D
CBCT scans were recorded. Thereafter, the anterior
and posterior sections of the diagnostic stent
were assembled on the maxillary cast modified earlier, and a second scan was made. Both these
scans were then utilized for the final treatment
plan. A customized surgical template (Quick
guide, Nobel Biocare) was fabricated accordingly
(Fig.2c), to assist the implant placement ensuring
the optimum inclination and alignment enhancing
the final prosthetic outcome. A provisional denture
was fabricated prior to the surgical procedure
using heat cure acrylic resin for immediate
provisionaliation post implant placement.
Following the routine protocol before implant
placement, 500 mg amoxicillin was prophylactically
given to the patient 1 h before surgery and rinsing
was done with povidone iodine mouth rinse.
Surgical site and adjacent area was scrubbed with
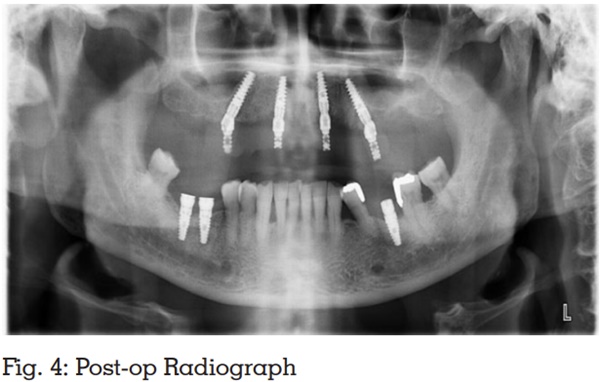
betadine. Infiltration anesthesia was given. After
profound anesthesia, the anterior maxillary teeth
were luxated and extracted atraumatically (Fig.3a),
following which the surgical template was tried and adapted to the maxillary edentulous arch with
the help of orientation pins of the guide (Fig.3b).
According to the manufacturer’s guidelines (All-on-Four procedures and products, manual No.
16896 Lot GB 0603, Nobel Biocare Services), to
avoid counter sinking, the implant sites were
underprepared thus increasing cortical bone
support. Four implants of dimensions 4.3x15mm
each (NobelActive, Nobel Biocare, Switzerland)
were selected for the anterior as well as the posterior
regions of the maxillary arch. Following implant
placement, final implant torque was checked with
a surgical torque wrench and verified with the ISQ
values. Multi-unit, straight abutments for anterior
implants and 35° angulated abutments for the
posterior implants along with titanium cylinders
(Fig.3c), were connected post the implant placement
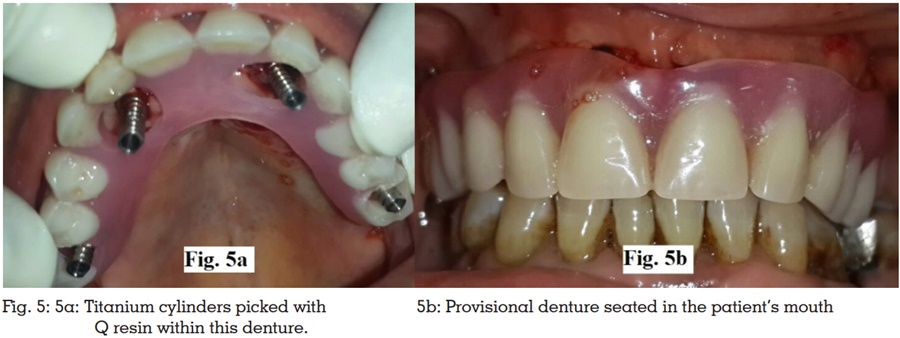
and tightening was achieved upto 35 Ncm with a
manual torque wrench. A post-op radiograph was
done to verify the alignment of implants and the abutments (Fig.4). The prefabricated maxillary
provisional denture was then seated and modified,
and titanium cylinders were picked with Q resin
within this denture (Fig.5a). This provisional
denture was then finished & polished and was
seated in the patient’s mouth the same day
(Fig.5b). For the rehabilitation of missing teeth
in the mandibular arch, a conventional implant
placement procedure was followed. Routine follow
up visits were scheduled at 1 week, 1 month and
3 months after the surgical procedure and steps
for fabrication of final prosthesis were initiated at
3 months appointment (Fig.6).

Full arch rehabilitation in patients is always
demanding functionally as well as esthetically. The
All-on-4 treatment concept optimizes the available
bone and allows for the rehabilitation of edentulous
jaws, eliminating the need of a bone graft, in one
surgical step through the placement of 4 implants-two anteriorly and two posterior implants angled
between 30-45 degrees commonly placed anterior
to maxillary sinus. The main objective of an all-on-4 approach is to obtain bicortical anchorage for
functional loading. Restoration of posterior atrophic
maxilla with a traditional implant supported
prosthesis demands bone grafting, sinus or ridge
augmentation procedures as an adjunct. However,
increased cost as well as the treatment time along
with additional surgeries and comorbidities
associated with these procedures calls for a
more safer and predictable alternative. Tilting
the posterior implants eliminates the requirement
of the above mentioned surgical adjuncts along
with increasing the anterior-posterior (A-P) spread
thereby shortening the cantilever, which along with
the cross-arch stabilization, enhances the implant/
prosthetic outcome. Use of longer implants can be
employed further enhancing the load distribution.
Angulation of distal implants in a 30 to 45 degree
position relative to the occlusal plane allows the
final prosthesis to have 10 to 12 teeth per arch.9
To minimize the cantilever, the posterior osteotomies
should be started as posterior as possible allowing
a distance of approximately 4mm from the anterior
wall of the sinus. The posterior osteotomies are
tilted to the maximum angle to the 45°, so that the
posteriorly tilted implants are placed a minimum
2mm anterior to the anterior wall of the sinus.
Achieving this precise angulation along with
the bicortical anchorage can be challenging
especially in the maxillary arch and requires
skill and expertise while performing a free hand
surgery. A fully guided surgery avoids these risks
and makes the surgical procedure more controlled
and predictable with desired prosthetic outcomes
improving the overall success rate of the final
prosthesis. It accomplishes a precise diagnosis
as well as a meticulous treatment planning and
provides for an accurate and precise implant
placement minimizing the likelihood of errors and
reducing the overall treatment time.10 Utilizing
the available bone to obtain the optimal primary
stability helps in immediate functional restoration
of the dental function. Immediate provisionalisation
can be implemented following achievement of
primary implant stability of 35Ncnm or higher.
Immediate rehabilitation improves the patient
acceptance of the final prosthesis, functionally
and esthetically.
Rehabilitation of edentulous arches with All-on-4
technique is a predictable treatment modality with
excellent success rates with a high survival. Overall
hygiene is also improved owing to the spread of the
four implants. In this technique we have made use
of a 3D planning and fully guided surgery for the
All-on-4 procedure in the maxillary arch followed by
immediate provisionalisation, complementing the
advantages of each one of these. The final result
being a more precise technique with less risks. In
totality, this technique demonstrated exceptional
aesthetic outcomes, without any complications,
with a reduced treatment time.