BACKGROUND AND OBJECTIVES: The comparison
of crestal bone loss in relation to implants placed
using conventional drilling osteotomy method and
using bone expansion screws in maxillary region.
METHODS: The crestal bone loss was measured
after implant placement and after a period of six
months, and the results analyzed. Equal number
of male and female patients of comparable age
group who opted implant treatment were selected.
RESULTS AND DISCUSSION: After a period of six
months of implant placement, a mean value of 1.37
mm of crestal bone loss was noticed for implants
placed using conventional osteotomy method while
a mean of 0.73 was noticed in relation to implants
placed using expansion screws.
CONCLUSION: The implants placed using bone
expansion screws show less crestal bone loss
compared to implants placed using conventional
osteotomy method in maxillary edentulous ridge
having less than ideal bone width. It infers that the
bone expansion method using expansion screws
is more reliable and relatively noninvasive way of
implant bed preparation.
Key words: Crestal bone level; Conventional osteotomy; Bone expansion screws; Implants.
Over the past few decades, removable dentures
have given way to fixed prosthetic options due to
the demand for esthetics and comfort. The major
breakthrough; the concept of “osseointegration” in
dentistry by Dr. Per Ingvar Brånemark1
along with
continued research benefited in the rehabilitation
of edentulous patients.
In the maxillary region, the advanced resorption
of alveolar bone and relatively lesser bone density
poses a challenge for implant placement. Many
techniques have been tried for widening edentulous
ridge, including osteoinduction2,3 osteoconduction4
,
onlay block bone grafting, alveolar distraction
osteogenesis5
, guided bone regeneration and
splitting to expand the ridge6,7. They come with
limitations including harvesting bone from oral
sites, highly technique sensitive, lower patient
compliance and increased morbidity.
Less invasive techniques using osteotomes and
bone expansion screws help to shorten treatment
length, avoid additional surgical appointments,
reduce trauma to patient and conserve the
maximum amount of alveolar bone and decrease morbidity8
. Bone expansion screws utilize a
thread former configuration allowing expansion
and lateral condensation of bone, when used
in increasing diameters inserted with a torque
wrench. They allow ‘corticalization’ of the implant
site which is advantageous for the primary stability
of implants in rather cancellous bone of maxillae
according to Lekholm & Zarb9
(1985).
This study was aimed to compare the crestal bone
loss which occurred in relation to implants placed by
‘bone spreading technique using bone expansion
screws with conventional method of osteotomy
preparation. Both methods are employed for
placing implants in edentulous ridge with enough
bone height as well as a minimum required width.
Estimation of peri-implant crestal bone loss is an
important parameter for evaluation and prognosis
of implant success10.
It is an observational clinical studyconducted
according to the guidelines of the localethical
committee of Thiruvananthapuram dental
college(IEC/E/4/2016/DCT/dtd 06/12/16).
This clinical study included patients with healthy
remaining dentition, good oral hygiene, no
retained roots/pathologic lesions, adequate inter-arch clearance, adequate quality and quantity
of bone, no known systemic disease, availability
for follow-up. Patients with smoking habit/drug
or alcohol abuse, Radiation treatment to head
and neck, ongoing chemotherapy, pregnant
and lactating women, post-menopausal
women, patients under corticosteroids and
immune-suppressants, Patients reporting after
recent extraction (less than 3 months) were
excluded.
Total sample size was 30. Consecutive cases
satisfying inclusion and exclusion criteria were
selected till the sample size was achieved. The
patients were given written information regarding
the risks of implant surgery and their written informed consent was obtained.
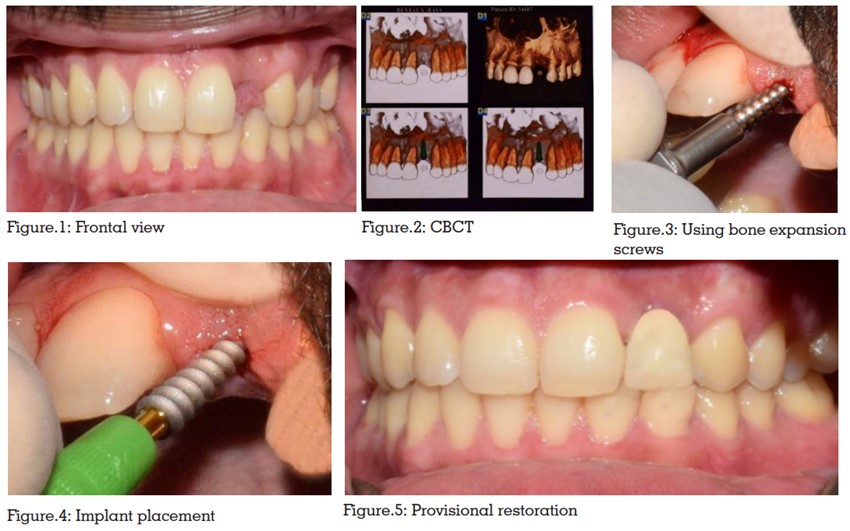
Based on the evaluation of diagnostic casts and
CBCT (Figure 1,2), titanium root form implant
(GenXT) dimensions were determined for each
patient. A safe distance of minimum 2mm was kept
from anatomical structures such as maxillary sinus.
The surgery was done under antibiotic coverage.
Betadine solution (5%) was used to disinfect the
extra-oral as well as intra-oral tissues. The patient
was asked to rinse with 1.2%mg/ml chlorhexidine
gluconate mouthwash for one minute. The site
of implant surgery was anesthetized by local
infiltration injection of 2% lignocaine with 1:200000
adrenaline (cadila pharmaceuticals).
Group A – Conventional osteotomy
method
Initial preparation was done using pilot drill
followed by sequential drilling using progressively
larger drills. The drilling was done using
physio dispensor under copious irrigation of normal
saline. The drill depth was assessed using depth
gauge. Once the planned implant diameter was
achieved, implant was placed with the help of an
implant mount.
Group B – Bone expansion screw
method
Pilot drill was used on the proposed implant site to
reach the desired depth. Bone expansion screws in
the order of increasing diameters were inserted into
the bone cavity. Screws of diameter 3.5mm, 4.0mm
and 4.5mm were used (Figure 3). A torque wrench
was used to insert the screw cautiously and slowly
upto the desired depth. The last screw spreader
used had to be slightly smaller in diameter than
the implant diameter. Implant was placed with
the help of an implant mount and inserted using
torque wrench (Figure 4).
In either of the above methods, immediate
loading single stage implants were placed in
each patient using immediate loading protocol.
An interim restoration was cemented on the day
of surgery after implant placement (Figure 5).
Digital periapical intraoral radiographs were
taken immediately after implant placement and
after six months (Figure 6). Regular clinical follow-up was done at one month, three months and six
months after implant placement.
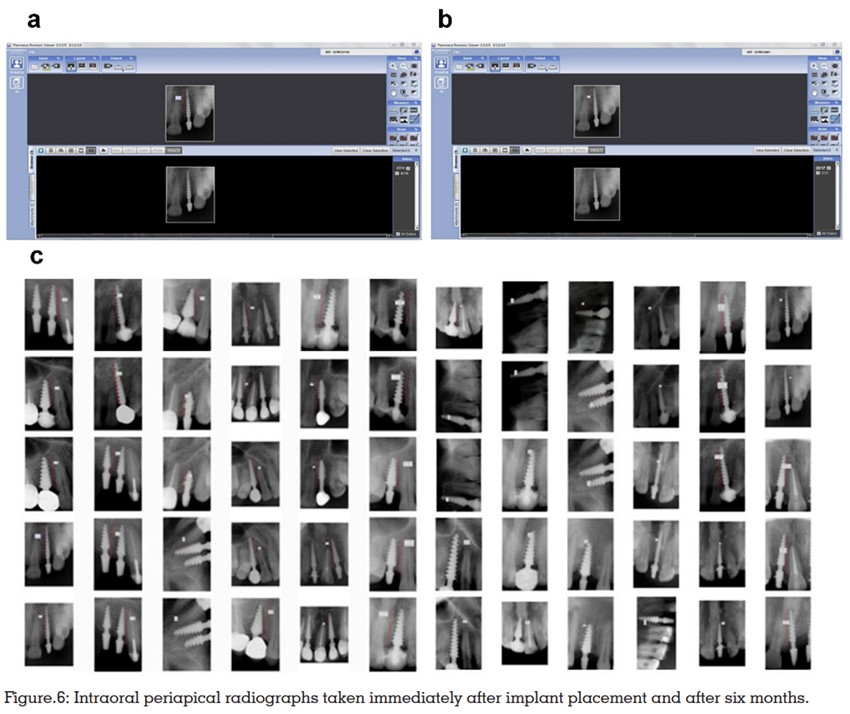
From the digital radiographs, the distance from
the mesial crestal bone level to the apex of the
implant was measured with the help of Romexis
software. The measurements were subjected to statistical analysis using Students t –test.
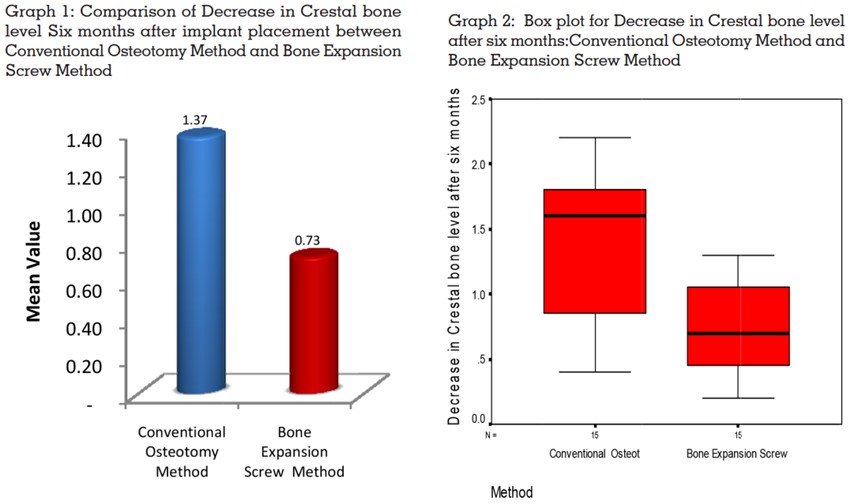
The crestal bone levels in relation to implants
placed using both methods were measured
immediately and after six monthsof implant
placement. Comparison of crestal bone level of
implants placed using both the methods were
measured immediately and after six monthsof
implant placement. After a period of 6 months of
implant placement, a mean value of 1.37mm of
crestal bone loss was noticed for implant placed
using conventional osteotomy method while a
mean of 0.73 was noticed in relation to implants
placed using bone expansion screws (Graph 1,2).
The study was significant at 0.01 level (Table.1.)
Though there are various surgical methods for
implant bed preparation, the conventional drilling
osteotomy technique has been the most used,
irrespective of the quality of bone. A scientific
backup of various studies shows consistent results
with good primary stability and success rate when
performed in good quality bone of adequate
volume11. But the removal of precious bone by
drilling is a major concern particularly in narrow
edentulous maxillary ridge of relatively poor bone
quality (D2, D3 or D4).
The present study was conducted to compare the crestal bone loss that occurred in relation to
implants placed using bone expansion screws,
with that of conventional osteotomy method using
bone drills. Crestal bone loss being an important
parameter for the evaluation of success of an
implant, it is possible to assess the reliability
of using bone expansion screws for implant
placement; which is a more conservative procedure.
Bone expansion screw method is primarily intended
for placing implants in edentulous areas with
sufficient bone height but insufficient bone width
as well as poor bone quality.
When it comes to implant treatment in narrow
edentulous ridges, there are numerous ridge
augmentation methods, but most of these surgical
procedures are invasive, involves risk of infection
and takes longer time period to reach their
goal7,12,13.
Bone expansion using screws and osteotomes
are two relatively atraumatic methods indicated
for implant bed preparation in edentulous ridges
of poor bone quality and inadequate width. The
concept of bone expansion screws was introduced
to overcome the shortcomings of osteotomes such
as the difficulty in controlling malleting force as
well as the risk of bone fracture. The screws can
be engaged into the receptor bone with the help of
a ratchet or torque wrench. With the introduction
of larger diameter screws, bone is pushed and
condensed laterally which allows a slow and
gradual expansion of the bone laterally rather
than losing bone by drilling.14,15 The implant should be 0.5 mm larger in diameter than the size of the
screw last used to expand bone16. The softer bone
quality found in type III and type IV maxillary bone
is improved by laterally compacting the medullary
bone16. The increased bone rigidity achieved by
bone condensation results in improved primary
stability of implants14. Patient compliance is also
more with this method16.
One of the drawbacks of using bone expansion
screws is that resilience of bone sometimes requires
revision of the osteotomies with final sizing drill
before implant placement. Also. a continuous
full turn in thin dense bone can lead to excessive
osteo- compression16. It can only be performed
in cases with cancellous bone within the cortical
bone on both sides17.
Immediate loading root form implants were
used for the study aiming at a shorter treatment
period with a stable and fixed long-term interim restoration on the day of surgery18. This treatment
option also aims at maintenance of the hard
and soft tissue contour and reducing the waiting
period18. The highly acceptable clinical success
rate of immediate loading implants has been
studied and proved by many pioneers like Maria
Chatzistauraw et al19 in 2003, Degidi M20, Piatteli
A in 2005, Cannizzaro et al21 in 2011, Yoo et al22
in 2006 etc.
Digital periapical radiographs taken immediately
after implant placement and six months later
were used for measuring crestal bone loss. The
measurements were made from the crest of the
bone to the apex of the implant with the help of
Planmeca Romexis software. Study by Penarrocha23
et al in 2004 shown that conventional periapical
films and digital radiographs were more accurate
than orthopantomography in the assessment of
perimplant bone loss. In order to reduce any bias
in technique, all the radiographs were taken by
the same person who is qualified and skilled for
the same.
In the present study, analysis of difference in the
crestal bone level in relation to implants placed
using conventional drilling osteotomy method
and using bone expansion screws immediately
after implant placement and after a period of
six months has been done. Descriptive statistics
along with Box plot was used to describe Crestal
bone level between two different methods at
immediately after and six months after implant
placement. Independent sample t-test was used for
the comparison of difference in crestal bone level
after six months between the two methods. For all
statistical interpretations. p<0.05 was considered
the threshold for statistical significance. Statistical
analysis was performed by using a statistical
software package SPSS, version 20.0.
After a period of six months of implant placement,
a mean value of 1.37 mm of crestal bone loss was
noticed for implants placed using conventional
osteotomy method while a mean of 0.73 was noticed in relation to implants placed using bone
expansion screws. The mean crestal boneloss
for Branemark implants has been determined to
be 1.5mm for the first year, followed by a mean
bone loss of 0.1 mm per year by Adell et al1
. This
value was confirmed by Cox and Zarb24 with their
5-year report.
The present study was statistically significant at
0.01 level. There is significantly lesser bone loss in
relation to implants placed using bone expansion
screws after a period of six months when compared
to implants placed using conventional osteotomy
using bone drilling. Here the implants were placed
in edentulous maxillary ridge which was classified
as belonging to D2, D3 or D4 type bone. Ridges
having a minimum of 4.5 mm width were included
in the study. The impression made can be that the
lateral bone condensation by bone expansion
screws improved the quality of porous medullary
bone of maxillae14. This technique conserved all
of the bone in the surgical site14,15. A study done
by Nishioka et.al14 in 2009 showed that the maxilla
with insufficient buccolingual width and relatively
less dense bone can be managed well by using
bone expansion screws.
Bone expansion screws allow the placement of
greater diameter implants than when conventional
method of osteotomy is used. Each 1 mm increase
in diameter of implant increases the surface area
by about 20–30%, which in turn decreases crestal
stress and eventually crestal bone loss11 Incidence
of green stick fractures are minimized and there
is no thermal injury to bone16.
The results of the present study indicate that
thread-former and “screw-type” design is more
appropriate for placing implants in areas of
buccal bone resorption and in soft maxillary
bone, than the conventional osteotomy drilling.
With proper patient selection, evaluation, pre-surgical planning, careful execution of surgical
technique and post-operative follow-up, favorable
results can be achieved. Long term data regarding the outcome and success rates would require
randomized studies to evaluate the predictability
of this technique.
Within the limitations of the study, the following conclusions were drawn after analysis of the results: