Pierre-Robin Sequence is a developmental
anomaly characterized by the triad of mandibular
micrognathia, cleft palate, and glossoptosis.
Neonates born with a cleft palate have difficulty
in feeding that is further complicated by nasal
regurgitation of food, excessive air intake,
choking and recurrent aspiration pneumonitis.
Due to difficulty in feeding, child’s growth can be
affected. To combat these problems, different feeding
interventions such as maternal advice and support,
modified bottles, Orogastric/nasogastric tubes
and feeding obturators, etc have been advocated.
However, there is evidence of delay in the growth of
children with a cleft as compared to those without
clefting.
The article describes the importance of measuring
growth parameters to evaluate the growth of cleft
palate patients.
Key words: Cleft Palate, Feeding Plate, Pierre Robin Syndrome
Cleft palate(CP) is a congenital abnormality of
the secondary palate and may be complete or
incomplete, unilateral or bilateral, or submucous.
The risk of developing orofacial clefts has
a multifactorial origin, whereby involving a
combination of genetic and environmental factors
like folate antagonists, anticonvulsants, White
non-Hispanic race, maternal first-trimester, heavy
alcohol consumption, maternal age, pre-pregnancy
diabetes mellitus, maternal smoking, and maternal
obesity.1
When infants have a cleft lip or palate, they have
difficulty creating negative intraoral pressure when
using a regular bottle and nipple. Unsuccessful
breastfeeding has been seen in babies with CL
and palate, due to dysfunctional musculature
including the lips, cheeks, tongue, velum, and
pharyngeal walls resulting in inappropriate oral
cavity sealing.2
Growth alterations or deficiencies are recognized in cleft palate patients, and needs proper
management. It is well recognized that in the
early months of life, children with clefts appear to
exhibit non-satisfactory growth. This deficiency in
growth maybe apparent at a later stage through
short stature or underdevelopment in weight.3
Feeding a child with Cleft lip and palate thus
establishing a successful feeding pattern is a
challenge for both the mothers as well as health
care professionals. A range of feeding problems
such as choking, gagging, excessive air intake,
and prolonged feeds, the entrance of milk in the
nasal cavity due to the short, fast, uncoordinated,
and ineffective intraoral suction can occur that
results in profound weight loss.4
The feeding plate obturates the cleft and restores
the separation between oral and nasal cavities.
It creates a rigid platform towards which the
baby can press the nipple and extract the milk. It
facilitates feeding, reduces nasal regurgitation,
reduces the incidence of choking and shortens the
length of time required for feeding. The obturator
also prevents the tongue from entering the defect
and interfering with the spontaneous growth of
palatal shelves towards the midline. It also helps
to position the tongue in the correct position to
perform its functional role in the development of
jaws and contributes to speech development. The
obturator reduces the passage of food into the
nasopharynx thus reducing the incidence of otitis
media and nasopharyngeal infections. The feeding
plate restores the basic functions of mastication,
deglutition and speech production until the cleft
lip and/or palate can be surgically corrected.5
Because of the increased frequency of infections
and feeding difficulties after birth there is a growth
lag in cleft children. In this article, we measure
the effectiveness of the feeding plate on growth
parameters. The pediatric protocol of care included
serial examinations in growth measurements
(weight, length, and head circumference).
A 2.5 months old male infant presented with a
history of cleft palate associated Pierre Robin
Syndrome with difficulty in feeding, recurrent
respiratory tract infection, and nasal regurgitation.
The mother reported that the baby is not able
to suckle milk properly and he was not gaining
weight. At the time of reporting the patient’s weight
was 2.7kg. (Birth weight was also same) There was
no history of craniofacial clefts in the maternal or
paternal family of the child. The pregnancy of the
mother was uneventful and there was no history of
previous treatment or surgery for the defect. The
patient was having micrognathia and glossoptosis.
Intraoral examination revealed a cleft in the soft
palate and uvula.
A feeding plate was made for this patient. The
infant’s mother was instructed about the method
of usage, function, cleaning, and maintenance of
the feeding plate. A regular follow-up of the patient
was done after 24 hours and 2 weeks follow-ups
were scheduled. During the regular follow-up,
neonate weight gain, height, waist, and head
circumference were measured.
Growth measurement techniques were
standardized. Weight was obtained by using
standard infant and toddler scales. The length was
measured with a horizontal anthropometer with
the child in the supine position. An anthropometric
tape that is flexible and non-extensible should
be used for measuring the head and waist
circumference of the patient. For measuring the
head circumference, the patient’s head is in the
Frankfort Plane (an imaginary line joining the
upper margin of the external auditory meatus and
the lower border of the orbit of the eye). The tape
was passed around the head and placed on the
most anterior protuberance of the forehead and
the most posterior protuberance of the back of the
head (we aimed to measure the maximum head
circumference).
For measurement of waist circumference firstly the
lower rib margin was palpated (costal margin)
and marked with a short horizontal line then the
iliac crest was palpated and marked with a short
horizontal line. Using the tape measure, the mid-distance between the two horizontal lines was
measured and was marked with another short
horizontal line in the middle. The tape was passed
around the waist, making sure it was in level and
positioned at the mid-distance mark on both sides.
Measurements were made at the end of expiration.
Three measurements were taken for both head and
waist circumference. Mean (average) measurement
was recorded by adding the values together and
dividing them by three.
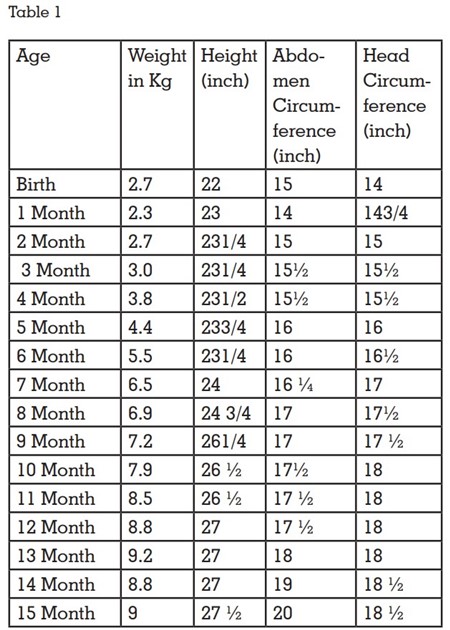
Length, weight, and head circumference were
measured at each examination. During the one year follow-up patient’s weight and height, waist,
and head circumference was increased and, in
that duration, no history of recurrent infections
was observed. (Table 1)
Pierre Robin syndrome(PRS) is a congenital
condition of facial abnormalities in humans. The
three main features are cleft palate, retrognathia
(abnormal positioning of the jaw or maxilla), and
glossoptosis (airway obstruction caused by the
backward displacement of the tongue base).
Pierre Robin sequence may be caused by genetic
anomalies at chromosomes.6
Primary care plays a vital role in these patients,
who often have numerous health care needs,
including feeding difficulties, speech disorders,
chronic ear infections, and dental & orthodontic
problems. The early repair of the palate is
associated with good cosmesis, better feeding,
adequate velopharyngeal competence, and good
speech & hearing development. The presence
of a congenital anomaly affecting the orofacial
structures such as cleft lip or palate, or both, maybe
thought to have an adverse influence on the growth
status and achievement of subjects affected with
such an anomaly. One might expect that the more
severe the cleft type, the more effect it may have
on the physical development of these patients.7
A regular follow-up of the infant is required for the
examination of oral mucosa which is very delicate
and easily damaged by the obturator. Also, check
up every 3-4 weeks at which the bilateral sides of
the border are reduced to accommodate growing
arches. A new obturator should be constructed
every three months to accommodate the enlarged
craniofacial sutures at growth. The mother should
be advised to hold the infant in an upright or
semi-upright position in feeding state so that the
swallowed air can be expelled during the feeding
process.8
Comprehensive management of children born with
cleft lip and palate is best accomplished by the
multidisciplinary team approach. Dentists play
an important role in the team which is working
closely with medical and allied health specialties.
However, prompt intervention by fabrication
of feeding plate can eliminate the immediate
problems i.e., proper nourishment and prevention
of infections for the already debilitated infant.9
Growth deficiency observed during this period has
been attributed to environmental factors including
the high frequency of infectious diseases and the
different degrees of difficulties encountered in
feeding children with cleft palate.10
The majority of studies demonstrated that children
with CLP presented with smaller body dimensions
when compared with typical children. Some
authors have suggested an association between
the severity of intrauterine growth deficiency
with the width of the cleft, with infants with CLP
presenting a greater risk for low-birth-weight birth
for gestational age.11
The growth of cleft patient has been improved by
the use of a feeding plate that has been evaluated
by the monitoring of growth parameters.