The loss of an eye in a child patient has a psychological impact on the growth and social acceptance. Replacement of the lost eye as soon as possible is necessary in such cases to enable the patient to cope better with the difficult process of rehabilitation. Here is a ten-year old child patient, who had undergone enucleation of her right eye due to carcinoma. After the enucleation patient was not using any prosthesis for a period of five years. Hence, initially the enucleated eye socket was restored with a modified stock ocular prosthesis followed by its replacement with more definitive custom-made ocular prosthesis. Thus emphasizing that, cosmetic rehabilitation with the help of ocular prosthesis of an appropriate size, colour and contour can prove to be of value functionally as well as aesthetically. The prosthetic eye promotes physical and psychological healing for the child patient and improves the social acceptance.
Key words: Ocular prosthesis, eye prosthesis, maxillofacial prosthesis
The disfigurement associated with loss of an eye
can cause significant physical and emotional
problems.1
The importance of an ocular prosthesis
with acceptable aesthetics and reasonable motility
in restoring normal appearance in patients with
anopthalmia has long been recognized. Most
patients experience significant stress, primarily
due to difficulty in adjusting to the functional disability caused by the loss of eye and to societal
reactions to the facial impairment.2
The loss of
an eye in a child patient has more psychological
impact on the growth, development and social
acceptance. Replacement of the lost eye as soon
as possible is necessary in such cases to enable
the patient to cope better with the difficult process
of rehabilitation.
The aetiologies of eye loss include malignancy,
infection and trauma.3,4 In case of malignancies
enucleation of the affected eye may be required.
Enucleation is the surgical removal of the globe
by severing all muscles, nerves, and blood vessels attached to it and a portion of the optic nerve
from the orbit. Enucleation is often considered
the treatment of choice for primary intraocular
malignancies, because it permits histopathologic
examination of the intact globe, as well as determination of intra neural or extrascleral spread of
the disease.5
Treatment for enucleated eye socket consist of
ocular prosthesis. The ocular prostheses are either
readymade (stock) or custom made. A definitive
technique for fabricating artificial eye using acrylic
resin was developed by the United States Naval
Dental and Medical Schools and was published
in 1944.6
Now several methods for the fabrication
of ocular prosthesis have been described in the
literature. Methyl methacrylate resin is the material of choice as it is superior to other ocular prosthetic materials in tissue compatibility, aesthetic
compatibilities, durability, colour permanence, adaptability of form, cost and availability.7
A multidisciplinary management and team approach
are essential in providing accurate and effective
rehabilitation and follow-up care for the patient.
Therefore, the combined efforts of the ophthalmologist, the plastic surgeon and the maxillofacial
prosthodontist are essential to provide a satisfactory ocular prosthesis.8
The aim of the article is
to present a case report of pediatric patient who
was rehabilitated with ocular prosthesis for her
enucleated right eye.
Case history and Etiology: A ten year old female
patient was referred to the Department of Prosthodontics from a private ophthalmologist for
the replacement of her missing eye. Patient gave
history of enucleation of her right eye for the treatment of carcinoma five years ago. Patient was
not aware of the type of carcinoma/malignancy
due to which the enucleation was performed. The
records could not be traced as the surgery was
done somewhere else. The ophthalmologist was
planning for another surgery as there was lesser
space available due to postsurgical soft tissue
contracture, making any prosthetic replacement
difficult. But the child’s parents were not willing
for any kind of surgical intervention. Thus the
ophthalmologist had provided her with a stock
conformer two months back before referring her to
the department. Patient was using the conformer
sparingly due to discomfort and pain on insertion.
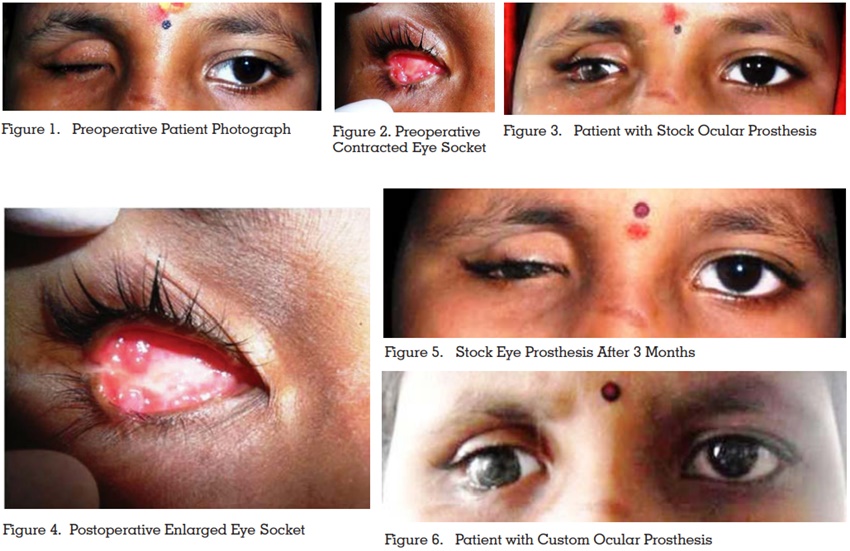
Clinical evaluation: On examination, The eye
lashes looked drooping and even the eye brows
looked unsupported because of the lost tissue support. The child was unable to open or close, and
perform any kind of movement with affected eye.
There was a gross facial deformity easily recognizable due to the lost eye.[Figure 1] The socket
looked depressed compared to the normal eye.
Though it was healed and the surrounding tissues
appeared normal, but the socket indicated a soft
tissue growth on the lateral canthus region. And
the depth of the socket was less for rehabilitation
with the ocular prosthesis. [Figure 2] This could
be attributed to not replacing the socket with any
kind of conformer or prosthesis to maintain the
space of enucleated tissues, since past five years
after the surgical procedure.
Fabrication of the ocular prosthesis: Though custom made prostheses are ideal for many cases,
a stock modified ocular prosthesis was chosen
initially for this case due to the lack of space. The
patient was explained the procedure for fabricating the ocular prosthesis and consent obtained
from her parents. For the impressions, the patient
was positioned in semi supine position in the
chair and trained in maintaining a fixed gaze on
a point directly in front of her and in a midline
position. A piece of tape placed on the wall at thedesired spot aided the patient in maintaining the
correct line of vision. The patient was instructed
not to move the eye or blink during the setting of
the impression material. The light body addition
silicone syringe material was loaded and injected
in the enucleated socket. When the impression
material was hardened it was gently removed,
checked for air bubbles and a cast was poured.
Using the cast a wax pattern was made and a stock
eye was trimmed appropriately and centred on
this wax pattern, and tried in the socket. After the
try-in of the wax pattern the ocular prosthesis was
invested, processed and finished. The prosthesis
was polished to a high gloss, thoroughly cleansed
with a brush, mild soap and water.9
The prosthesis was inserted in the patient’s enucleated eye socket and examined for esthetic appearance. [Figure 3] The iris colours were matching
and the patient did not experience any difficulty in
the socket. The patient was quite happy with her
restored aesthetics. Patient was given instructions
on the use of the prosthesis. The parents were also
instructed how to remove and insert the prosthesis
manually. Patient was instructed to wash the prosthesis with pure soap and tepid water, scrubbing
it well between thumb and fingers and rinsing it
well before reinsertion. The patient was evaluated
three days after the insertion and she did not have
much difficultly with the use of the prosthesis. She
was instructed for regular recall visits.
In regular recall visits over a period of 3 months
patients restored eye socket was evaluated for
increase in its dimension in terms of depth and
width due to the insertion of stock ocular prosthesis.
And it was found that considerable changes took
place in socket size due to the continuous use of
the prosthesis. [Figure 4] Hence when the socket
size increased adequately and stock ocular prosthesis became loose fitting, decision was made to
fabricate a new ocular prosthesis. [Figure 5] At this
stage because of presence of adequate space in
the socket, custom ocular prosthesis was fabricated
with the similar impression procedures mentioned above. Once the wax pattern was prepared, this
time only the iris portion of the stock eye was
trimmed and positioned in the centre of the wax
pattern and trial insertion was done. Fabrication
procedures were followed as mentioned above.
Newly fabricated prosthesis was custom made
hence, it had a better adaptation and because
of the increased size of socket aesthetic outcome
was excellent compared to the earlier prosthesis.
[Figure 6] As the growth of the child continues and
socket continues to increase in size, fabrication
of such ocular prosthesis has to be repeated after
every 6 months to 1 year duration.
Enucleation results in enophthalmos and sulcus
defects. A fundamental objective when restoring
an anopthalmic socket with an ocular prosthesis
is to enable the patient to cope better with the
difficult process of rehabilitation.10 Hence, a temporary conformer to prevent tissue contraction will
maintain proper contours. Early replacement of
the conformer by an ocular prosthesis allows for
cosmetic rehabilitation and improved quality of life.
Empirically fitting a stock eye, modifying a stock
eye by making an impression of the ocular defect
and the fabrication of custom eye are the most
commonly used techniques. Though a custom
ocular prosthesis has several advantages such
as intimate contact between the prosthesis and
tissue bed, and equal distribution of forces, it is
contraindicated when an undue change in socket
volume has taken place such as micropthalmos
or tissue shrinkage due to non compliance in the
use of ocular prosthesis by a growing child. Hence
socket expansion with the use of stock ocular prosthetic device of progressively larger size over an
extended period of time gives promising results.
The stock ocular prostheses can be easily modified in the dental office with available materials. If fabricated properly the prosthesis can provide
satisfactory fit and esthetics to the patients. In
case of pediatric patients such prosthesis would
be of immense use due to its easy fabrication and
limited number of visits required.
I have lost my one eye from long time, eye specialist had given me an artificial conformer to wear in
the lost eye but I did not use it because it used to
hurt. In my school also other kids used to tease me,
even they used to point the finger towards me. My
teachers also keep asking me how I lost my eye,
hence I was reluctant to go to school. But when I
got artificial eye, many people could not recognize
that I don’t have one eye. Even my school friends
could not recognize which one is the artificial eye
and which one is the natural eye. I use artificial
eye regularly and now I am habitual to wearing
it and removing it on my own.