
Dr Prasanth V
Editor
Data and Variables
We often note the name, age and gender of our
patients in case record forms. Most of the people are
bothered about their body weight. All these attributes
are called ‘variables’. A variable is simply what is
being observed or measured. In other words attributes
of patients and clinical events that vary and can
be measured is called as a ‘variable’. As the name
implies, variables vary among the members (units of
observation) of a ‘population of interest’ and if they
don’t vary, they become ‘constants’. In ‘165 centi-meters
of height’, ‘height’ is the variableand ‘165 centimeters’
is the data. Statistics addresses variability.
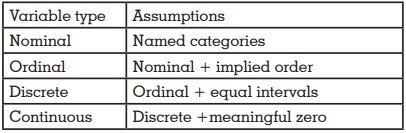
Variables are classified in many ways. Basically they
are either ‘qualitative / categorical’ or ‘quantitative’
in nature . ‘Qualitative’ variables can be ‘nominal’,
‘binary/dichotomous’ or ‘ordinal’. Nominal variables
are just named categories with no implied order
among them. Gender, type of removable prosthesis
delivered etcare examples of nominal variables
because it doesn’t matter whether we say male or
female first and it doesn’t matter whether we say
Removable Partial Denture or Complete Denture
first. ‘Binary or dichotomous’ variables are a type
of ‘nominal variables’ where there are only two
mutually opposite and exclusive options like ‘yes/no’
or ‘live/dead or ‘prosthesis present/absent’. ‘Ordinal’
variables on the other hand have an implied order
unlike ‘nominal’ variables, but the difference between
successive categories may not be equal. Stages
of cancer and type of bone quality are classical
examples. Cancer staging according to severity is
expressed from Stage I to Stage IV, we can’t say
stage IV before stage II. But the difference in severity
between Stage 1 and II may not be same as the
difference between stage II and IV. ‘Quantitative’ variables are measured in numerical values and
they can be either ‘discrete’ or ‘continuous’. If data is
available only in fixed intervals of whole numbers,
variable is of ‘discrete’ type. Most of the scales like
GCS, IQ, number of teeth present etc are examples of
discrete variables. Even though the difference between
successive categories are the same, true or meaningful
‘zero’ value may be absent here. Temperature in
degree Celsius is a classic example. Zero degree
Celsius doesn’t mean there is no temperature (it is
the temperature at which water freezes) and hence 50
degree Celsius is not the half of 100 degree Celsius, but
the difference between 25 and 50 degrees are same as
the difference between 50 and 75 degrees. Hence we
can say that only addition and subtraction are possible
if variable is ‘discrete’. But if data can be obtained in
continuum, variable is termed ‘continuous’. Examples
include height, weight, fasting blood sugar, available
bone etc. Here addition, subtraction, division and
multiplication of data values are meaningful simply
because there is a true and meaningful zero. 0 Kg
weight means, there is no weight and 50 Kg is exactly
the half of 100 Kg.
Continuous data is the most superior form of data
followed by discrete, ordinal and nominal. We can
always downgrade a data, but upgradation of data is
normally not possible. Always try to collect the data in superior form. For example, when you are collecting
the age of study participants, collect the exact age in
years, months and days (as continuous) and never
as completed age (as discrete)or age groups (as
ordinal). This is because we can convert continuous
data to discrete or ordinal if and when needed, but
we can never do a reverse process. Nominal variables
are measured in ‘nominal scale’, ordinal variables in
‘ordinal scale’, discrete variables in ‘interval scale’
and continuous variables in ‘ratio scale’. High ordinal
variables (semi quantitative variables) like GCS
categories can be analyzed in interval scale. As a
general statement we can say that the nominal or
ordinal data are restricted to ‘non-parametric’ statistics.
Variables can be ‘dependent’ or ‘independent’.
Outcome of interest which changes in response to our
intervention is called ‘dependent / outcome’ variable.
The factor which s manipulated is called ‘independent/
exposure/predictor’ variable. ‘Dependent’ variables
change in response to ‘independent’ variables. If we
assess the crestal bone level six months following the
osteotomy using conventional and bone expansion
techniques, crestal bone level is the dependent
variable and the two techniques compared become
independent variables. But if we study the relationship
between crestal bone level and implant failure, crestal
bone level will become the ‘independent’ variable and
implant failure, the ‘dependent’ variable. Now you may
have understood very well that the same variable can
become dependent or independent variable depending
on the research question or on what you really study.
If dependent variables are mediated through a third
set of variables, the latter is called ‘intermediate
variable’. For example, in case if crestal bone height is
mediated through gingival inflammation, then gingival
inflammation becomes the ‘intermediate’ variable.
A more explanatory example will be the study on
coronary heart disease resulting from increased salt
intake which is mediated through hypertension.
Salt intake → hypertension → coronary heart disease
(Independent) (intermediate) (dependent)
Variables can be ‘composite’ or ‘baseline’. It is logical to understand and height and weight are ‘baseline’
variables and BMI which includes both height and
weight is a ‘composite’ variable.‘Hard outcome’
variables like death, complete connector fracture etc
do not result in any bias. ‘soft outcome’ variables like
pain, peri implantitis etc are difficult to measure and
hence can result in bias. Condition of liver can be
directly assessed by a biopsy. But most often we resort
to liver function tests to indirectly assess its status. Liver
enzyme value, thus is a ‘proxy variable’.
Other variables, may be part of the system under study
and may affect the relationship between independent
and dependent variables are known as ‘extraneous
variables (covariates)’. They are called so because they
are extraneous to the research question, but may be
part of the phenomenon under study. Few covariates
can even be ‘confounders’ or ‘effect modifiers’. In depth
discussion on those topics will be beyond the scope of
this editorial.
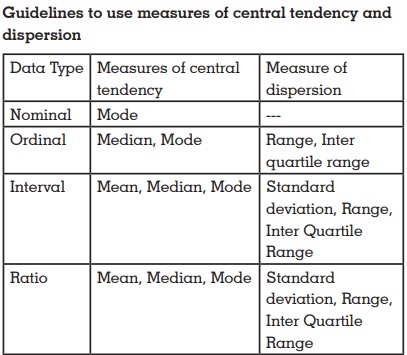
Why identification of variables is important?
Descriptive and inferential statistical methods used
are different for different types of variables. Summary
measures used, graphical representations used and types
of statistical tests used are unique for each type of variable.
Bar diagrams and pie charts are useful for
summarizing qualitative data. Histograms, frequency
polygon, leaf and stem plot, box plot, scatter plot
etcare useful for quantitative data. McNemar’s chi
square test is useful for qualitative paired variables.
Paired t and RM ANOVA are useful for quantitative
paired variables withWilcoxon Signed Rank test and
Friedman’s test being their non-parametric variants.
Chi square test and correlation are used for unpaired
qualitative and quantitative variables respectively.
ANOVA and its two sample version, unpaired t test are
useful for comparison of sample means. Less robust
Z test which is based on stronger assumptions can
substitute unpaired t test,only is sample size is large.
Mann-Whitney U test and Kruskal Wallis H test are the
non-parametric variants of unpaired t and ANOVA
tests respectively.
Even though concept of variables and data are
important in research,sometimes we may interpret few
datainter changeably. For example, IQ, which is most
likely an ordinal variable is interpreted as interval
variable by most. Like Geoffrey R. Norman and David
L. Streiner stated ‘as far as we know, they have not
been arrested for doing so, nor has the sky fallen on
their heads’.
Test your knowledge
Systolic BP – Continuous (though we collect as discrete
values)
Age group – Ordinal (there is an order)
Completed age – Discrete (always a whole number)
Age – Continuous (need not be whole numbers)
Gender – Nominal (we can say any gender first)
BMI Categories – Ordinal (there is an order)
Rank in exam – Ordinal (Even though rank is given
as 1,2,3….., it’s just a number to denote an order of
merit. Rank 2 doesn’t mean that he/she has only half
knowledge/mark than Rank 1)
RBC Count – Discrete (only whole numbers are
possible)
References