The loss of a finger can adversely affect the patient physically and psychologically. Most common causes being trauma, congenitally missing or deformities. Such deformities can be rehabilitated prosthetically by means of adhesives, vaccum retained or ring retained prosthesis. An osseointegrated digital prosthesis offers better retention than the other methods. This article describes the rehabilitation of an amputated thumb with implant retained silicone prosthesis to restore the patient’s physical, mental and social wellbeing.
Key words: Finger prosthesis, osseointegrated, bicortical implant
The absence of human body parts by trauma,
diseases or congenital deformities lead to altered
function, sensation and image. One of the most
common examples of such situation in the industrial
world is the loss of fingers that can cause the
above impairements.1,2 Today, several surgical
and microsurgical techniques are available for
the repair of damaged fingers when the victim
approaches the hospital soon after the incident.
When surgical methods not possible, due to some
reasons, an esthetic finger prosthesis is a blessing to handle the defect.3
Retention is the primary determinant factor in the
success of a prosthesis. Various methods have been
tried to retain a finger prosthesis, including vacuum
effect, adhesives, metal rings or other means.1,4
Nowadays implant retained prosthesis has got
wide acceptance over conventional methods when
the remaining structure has adequate bone. It
is possible to retain a prosthesis if the residual
finger stump measures 1.5cm or less.2,5 Implant
supported prosthesis not only shows superior
esthetics and comfort but also has the ability to
conduct tactile stimuli to the adjacent hard and
soft tissues.
This clinical report describes the use of a bicortical
implant to retain a silicone thumb prosthesis.
A 45 -years old male patient lost part of his left
thumb during carpentry work 3 months ago was
referred for artificial reconstruction of the lost
structure. Clinical and radiographic evaluation
revealed that the amputation was at the level of
the distal interphalangeal joint and wound healing
was satisfactory
The remaining bone measures 17mms and has good quality cortical bone. It was decided to place
an implant into the residual bone to which a silicone
finger prosthesis would be fixed. The treatment
procedures explained to the patient and a consent
was obtained. The width of the inner cortex and
the length of the bone to the subchondral area
were measured from the radiograph to determine
the dimensions of the implant (figure 1). A flapless
procedure was carried out under local anaesthesia
(digital block) and the distal part of the bone was
explored with a tissue punch and a drill hole was
made into the bone with a lance drill. The drill hole
was enlarged to a level of 3.2 mm by sequential
drilling. A one piece bicortical dental implant
(Bicortical, Oraltronics Dental Implant Technology
GmbH) of 3.5mm x 23mm with square post was
selected and was inserted in to the implant bed
prepared on the proximal phalanx. Radiographic verification was done (figure 2).
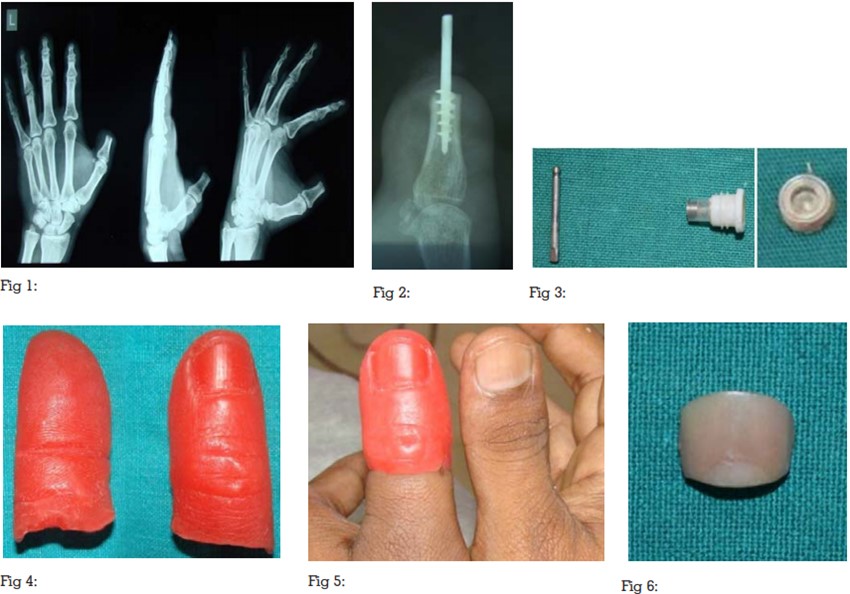
At the end of a 10-day healing period, the abutment
part of the square post was modified as a ball
head to receive a nylon O-ring on it (figure 3).
Impression was made using silicone impression
material (Flexceed; GC Dental Products Corp.,
Japan). Once the impression material had set, the
impression was removed,laboratory analogue
was placed and a working model was prepared
using Class-III dental stone (Kalstone; Kalabhai
Karson Pvt. Ltd., India). Impression of a person’s
thumb of similar shape and size was made using
irreversible hydrocolloid impression material
(Tropicalgin; ZhermackSpA) to which molten wax
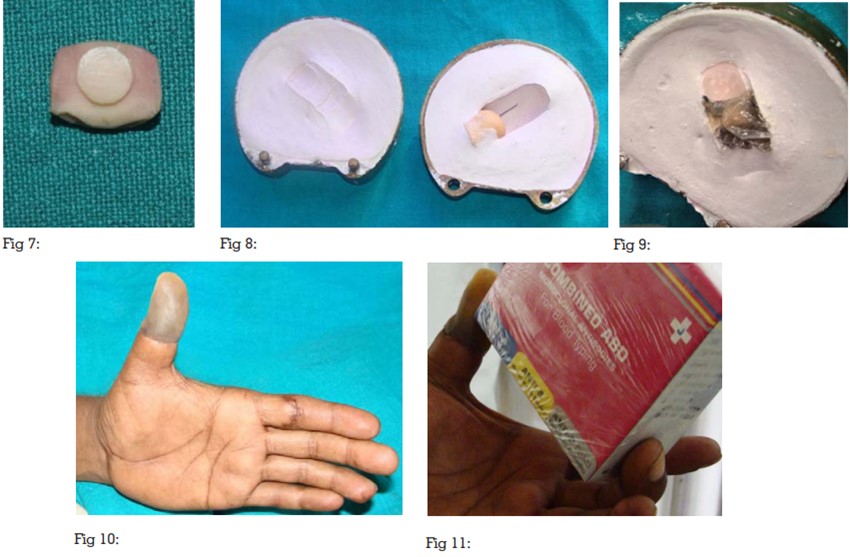
was poured to duplicate the lost finger. After
necessary modifications the wax finger (figure 4,5)
was then adapted on the working model and the margins were merged to the edges of the defect.
The nail was customized and fabricated with a
built in retentive element (figure 6,7), using self
–polymerising acrylic resin (DPI-self Cure tooth
moulding powder) and was incorporated into
the nail bed created on the wax model. It was
then flasked and dewaxed (figure 8). Different
shades of intrinsic colours were mixed with silicone
(Maxillofacial Rubber; Technovent) to match the
colour of the thumb (figure 9). The O ring was
securely placed over the implant analogue before
packing the material and the curing process
was performed according to the manufacturer’s
instructions. The prosthesis was retrieved from
the mold and finished (figure 10). Fine details
of color matching was done with extrinsic stains
and evaluated for fit. The patient could reproduce
the finger movements of the stump without
displacement of the prosthesis. The patient was able to grab and hold things as like normal thumb
(figure 11).
Home care instructions explained to the patient
which included mechanical debridement of the
skin around the abutments with a soft tooth brush
and irrigation with warm water and soap. Clinical
and radiographic follow up done 6 months post
operatively and did not reveal any complications.
Traumatic amputation of a finger can cause
physical and emotional difficulties. An aesthetic
prosthesis for the finger can offer psychological,
rehabilitative and functional advantages.6
Prosthetic rehabilitation of the finger restores the
body anatomy and allows the patient to expose
his hand with confidence.7
A precisely fitting
prosthesis is essential for this purpose.4
The prosthesis is attached securely by means
of an osseointegrated implant placed within
the intramedullary canal of the residual bone
of the amputated digit.5
ball and socket type of
retentive features provided optimum retention and
could be easily taken on and off by the patient.
The prosthesis was fabricated from silicone,
contributing to the satisfactory aesthetic results,
also feel like soft tissue.2
Partial recovery of the tactile sensation
(osseoperception) can be attained by using
implant retained finger prosthesis. Lundborg et
al. proposed that this occurs as a result of the
transfer of tactile stimuli to intraosseous nerves via
the osseointegrated implant.1
The patient is able
to perform daily manual activities such as holding
or grabbing objects like small boxes, cups, etc. In
the studies of Manurangsee et al. and Sierakowski
et al., patients scored highly in the Jebsen Hand
Function Test, with results close to the contra-lateral
hand.12,13 A restricted metacarpophalangeal joint
would restrain the adequate functioning of the
prosthesis.2
The placement of one piece implant
eliminated an additional surgical intervention,
shortened the treatment time and reduced the
trauma for the patient.14
Out of the available maxillofacial materials,
customized silicone prosthesis has a comparatively
larger acceptance rate due to their superior
comfort, esthetics, durability and stain resistance.
Few other added benefits of silicone prosthesis are
desensitization and protection of the hypersensitive
tissue at the amputation site, which is achieved
by the constant gentle pressure exerted over the
affected area.9
Fingers are quintessential in daily life. Apart
from their functional purpose, they also pay an
important part in human communication and
expressions. Amputation of fingers will result in functional deficiency as well as aesthetic problems.
An osseointegrated digital prosthesis addresses
both the issues and permits the patient to perform
daily activities and thereby eliminating the physical
and psychological trauma occurred to the patient
due to the loss of finger.