Restoring a missing tooth in the esthetic zone poses a challenging situation to the clinician. Amongst the various pontic designs proposed in literature, the most acceptable pontic design is the ovate and modified ovate design, that can be used both in immediate and delayed extraction sites. Before the final restoration is fabricated, adequate planning and laboratory communication is required so as to modify the provisional restoration and contour the soft tissue. The present case report provides a technique to condition the soft tissue around the pontic to provide an esthetically acceptable outcome.
Key words: sub pontic soft tissue, esthetic restoration, ovate pontics, soft tissue conditioning, contour, emergence profile, esthetics
One of the most challenging job for a restorative
dentist is to rehabilitate the missing tooth in the
esthetic zone. The pontic design must fulfil both
functional and esthetic replacement of the missing
tooth.1,2 Irrespective of being a conventional or
implant retained FPD, the pontic design must be esthetically acceptable, enable adequate oral
hygiene, should avoid tissue irritation and be able
to mimic the emergence of a natural tooth.3,4,5 It
should support the surrounding soft tissue and
interproximal papillae to produce an illusion of
emergence profile of a natural tooth.
In 1926, Brill designed and advocated the use of
porcelain root extension pontics into extraction
sockets to achieve optimal esthetics and hygiene
maintenance. Subsequently in 1933, Dewey and
Zugsmith advocated the use of Brill’s pontic design
for post-extraction sites.6
In 1980 Abrams designed
the all convex ovate pontic design in post extraction
sockets, to condition the soft tissue and by guiding
papilla growth and stabilization.7
Most often the
patient presents with a healed socket which has
soft and hard tissue deficiency occurring post
extraction. The ovate pontic contacted a larger
area of the underlying soft tissue and applied
light pressure on the ridge tissue, as compared
with the ridge lap or modified ridge lap pontic,
which were in passive contact with tissue without
application of pressure.1
Liu improvised the design of ovate pontic by
making it less convex with decreased labiolingual
thickness to more accurately duplicate emergence
profile.[8] This was called the modified ovate
pontic design.
A 35-year-old female reported to the Department
of Prosthodontics, with a missing maxillary left
central incisor. The patient gave a history of trauma
to the maxillary teeth during her childhood which
led to the subsequent loss.
The patient had high lip line and the smaller
occluso-gingival dimension of all anterior teeth
led to a highly pronounced gummy smile. She also
had internal stains in all her teeth akin to fluorosis
[Figure 1]. The overall gingival health was good
and the mucosa in the edentulous space was
thick and keratinized. Subsequent radiographs
revealed no underlying pathology.
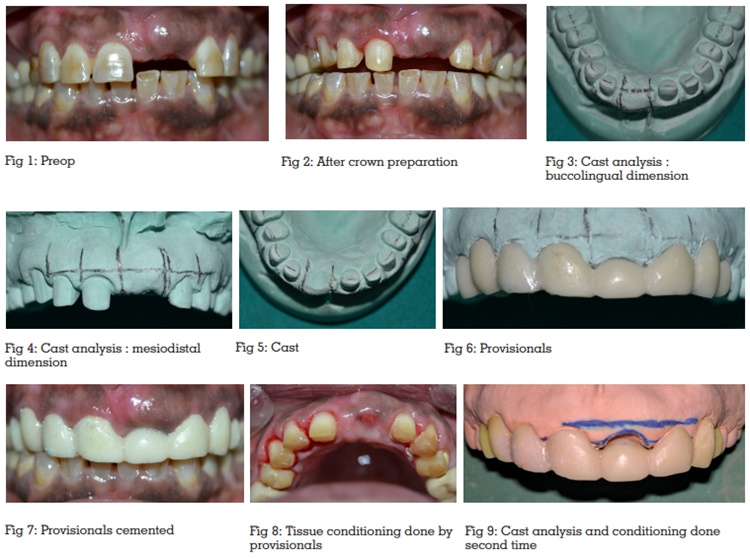
Study cast analysis revealed that the mesio-distal
width of the edentulous space of the pontic site
was almost double of the incisal-gingival height
present. The adjacent right central incisor and left
lateral incisor also revealed a major discrepancy
in proportion of their length as compared to
the width. The patient wanted a non-surgical
esthetically acceptable solution for the missing
tooth simultaneous with improvement in color and
appearance of her anterior teeth.
The treatment plan designed was to rehabilitate
the missing tooth with a three-unit bridge with an
ovate pontic. Individual crowns for teeth 12, 13,
14, 15, 24, 25 in order to improve the color (fluorosis
stains), the length to width ratio and proportion of all the anterior teeth. It was estimated that a
gradual conditioning of the soft tissue will require
a set of provisional with modified ovate pontic
design; so as to stimulate the growth of papilla
around the pontic and achieve desired esthetic
result.
Teeth preparation was done following all the
biomechanical principles and impression was
made using addition silicone impression material
in a stock tray. A working cast was obtained
subsequently and cast analysis was done.[Figure
2,3,4]. On the working cast, a shallow depression
of up to 2mm was created in the edentulous space
to allow fabrication of an ovate tissue surface for
the pontic and subsequently temporary crowns
were fabricated in auto-polymerizing tooth colored
acrylic [Figure 5,6]. The intaglio surface of the
temporary ovate pontic was polished to a smooth
gloss. The depression that was created did not
coincide with the dimensions of the final restoration; the goal was to slowly push and shape the mucosa
in increments so that better and predictable results
are achieved. Temporary crowns were luted using
eugenol free temporary cement [Figure 7]. This
approach allowed sufficient adaptation and
healing of the pressurized mucosa, leading to
stimulation of the papilla and decreasing the risk
of the mucosa getting receded. The patient was
given oral hygiene instructions and was recalled
the next day for evaluation of tissues around the
pontic site which was found to be healthy.
After 1 week, the temporary crowns were retrieved
from the patient’s mouth and a healthy ovate
depression was observed at the pontic site [Figure
8]. The same working cast was further modified by
deeping the ovate depression by approximately 1 –
1.5mm [Figure 9]. The temporaries were seated on
the cast, and the tissue surface of the ovate pontic
was relined with auto-polymerizing tooth colored
acrylic and was well-polished. The temporary crowns were checked and cemented [Figure 10].
A 24 hours follow-up was done. After 1 week the
procedure was repeated and temporary ovate
pontic was again relined, but, now to its final
dimensions [Figure 11,12]. A 24 hours follow-up
was done again.
After 3 weeks, the temporary crowns were removed.
The fully conditioned and completely shaped
ovate pontic site was inspected. It appeared to
be healthy and normal, thereafter, decision was
made to make the final impression [Figure 13,14].
A modified impression technique was used, to
accurately register the modified pontic site. Prior to
impression making, the existing temporary crowns
were duplicated in tooth colored auto-polymerizing
acrylic resin. The old temporaries were placed
on the prepared teeth and were picked in a putty
impression following which, the temporaries were
removed from the impression. The pontic was
detached from the rest of the temporary prosthesis
and was reseated in the putty impression. The putty
impression, with the temporary pontic in place,
was relined with light body impression material
and the impression was made [Figure 15,16]. The
new set of duplicated provisionals were cemented.
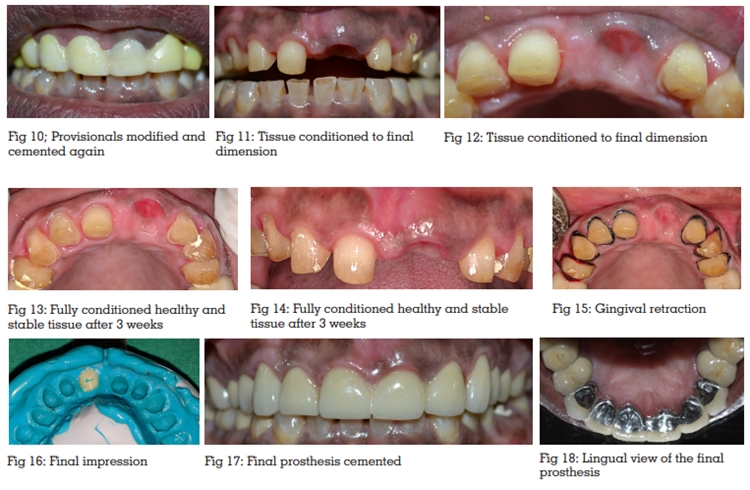
Master casts were prepared, face bow transfer
was done with subsequent articulation in a
semi-adjustable articulator. The final prosthesis
fabricated was a porcelain fused metal fixed partial
denture comprising of individual crowns for 12, 13,
14, 15, and 23, 24, 25 and a three-unit bridge for
11, 21, and 22. At the stage of bisque trial;occlusal
adjustments were done and patient’s opinion was
obtained. After glazing the final prosthesis was
luted and excess cement was removed using floss
[Figure 17,18]. The patient was educated about
hygiene maintenance. Follow up was done after
1 month,6 months and a year.
In the early twentieth century, bridges had porcelain root pontics extending into extraction sockets or
surgically prepared sites. This technique was
associated with poor oral hygiene, inflammation,
mucosal swelling and infections; therefore, it
consequently fell out of favour.
Stein’s work confirmed that mucosal contact
and pressure should be avoided. Thereafter, the
modified ridge lap pontic became the design
of choice. However, once the importance of
plaque control in maintaining mucosal health
was understood, clinicians began to revisit and
modify pontic designs.8
The ovate pontic has an all convex design making
it conducive for oral hygiene without compromising
esthetics. The intaglio surface of an ovate pontic is
convex, smooth, highly polished and maintains a
slight passive contact with the underlying mucosa.
The temporary bridge fabricated was used to apply
controlled pressure on the ridge area to develop
the desired contours of the pontic site without any
overt signs of inflammation.
Jaques had described a non-invasive tissue
sculpting technique which allowed for fabrication
of a pontic with adequate emergence profile and
pseudo interdental papilla.9
The technique used here differs from that developed
by Jaques in the way that, preparation of the pontic
site was done on the working cast after close
calculations of the dimensions, the relining of the
pontic’s tissue surface was done on the working
cast as opposed to Jaques’s technique which was
a chairside procedure.
However, a minimum 3 to 5 mm of soft tissue
thickness is required to achieve optimum results
so as to compress the tissue without surgical
intervention.10 The controlled pressure applied by
provisional restoration can be verified by ensuring,
that the blanching of soft tissue subsides within
5 to 10 minutes.11
The modified impression technique allowed the accurate transfer of the soft tissue contours.
Similar techniques were described by Winston W.
L. Cheeand Terry E. Donovan.12.13 This impression
technique also prevented the tissue rebound that
can happen once the provisional restoration is
removed and can create a pontic space that is
shallower than the intended dimensions.2
The main advantages of this technique were to
contour and replicate the interdental papilla almost
similar to that of natural teeth. Time allowed for
healing helps to verify esthetics and phonetics.
Daily hygiene practices provide continuous
moderate pressure against the apex of the pontic
and abutment connectors ensuring optimal tissue
health.
However, the procedure is time consuming and
involves multiple appointments. Attention to tissue
healing and existing provisional restoration is
necessary for an acceptable marginal fit.
Maintenance of oral hygiene by patient plays
critical role in success of the procedure.
The ovate pontic is an approach for esthetically
demanding anterior bridgework. An ovate pontic
design has an increased amount of mucosal
contact and applies light pressure to the underlying
mucosa in an attempt to improve esthetics.7
This
pontic design addresses the issue of emergence
profile esthetics, but its use must be combined
with effective oral hygiene procedures to obtain
a successful esthetically acceptable outcome.