AIM/PURPOSE: The purpose of this review article
is to compare the efficiency of hard and soft splints
that have been used to treat temporomandibular
disorders.
RESULTS: Both forms of occlusal splints (soft and
hard)improved temporomandibular disorders.
CONCLUSION: In spite of numerous disagreements
regarding the efficacy of occlusal splints many
studies proved that occlusal splints are the most
common and efficient treatment for TMD patients
with a success rate of 70-90 %.
The temporomandibular joint is referred to
as “ginglymodiarthrodial” ginglymoid means
rotation and arthroidial means translation. During
initial mouth opening condyle rotates followed
by translation. Temporomandibular joint should
harmonize with the different components including
mandibular condyles, meniscus, glenoid fossa,
ligaments, and muscles that is well documented.1,3
The function of TMJ is well maintained until it
is disturbed by external factors that affect the
joint function, such as mechanical, psychological,
occupational, and habits. Pain, clicking, noise,
grating in the jaw joint or problems in chewing or opening of jaw are the common signs and
symptoms of temporomandibular disorders.5,6
Anderson et al. reported that approximately 75%
of the total population manifest at least one sign
of joint dysfunction. This review article is intended
to evaluate the use of hard and soft splints as
a treatment modality for temporomandibular
disorders.
Reassurance (patient education, self-care and
behavior therapy), transcutaneous electric nerve
stimulation (TENS), occlusal splint therapy,
physiotherapy (such as ultrasound, acupuncture,
short wave diathermy laser, heat exercises, and
biofeedback) drug therapy, occlusal adjustment,
surgical intervention and combined treatment were
the numerous treatment options available today
Occlusal splint therapy has been frequently used
treatment modality for patients with sleep bruxism
to protect teeth from damage caused by forceful
jaw muscle contractions or to reduce orafacial pain,
if present. However, little knowledge is available
regarding the mechanism of the action of occlusal
splints.3,4,5 Most of the studies have examined
changes in the masticatory muscles activity before
and after application of an occlusal splint.
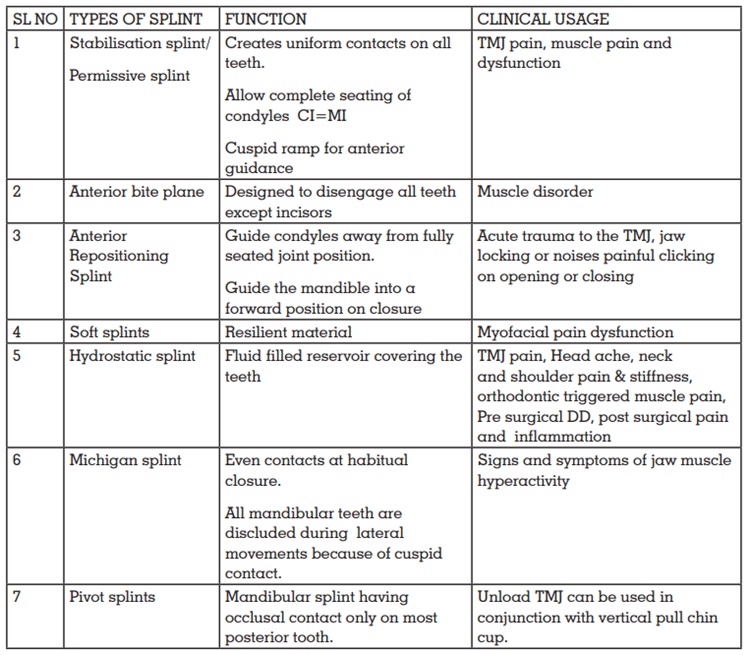
Okeson classified the occlusal splints as
stabilization appliance and anterior repositioning
appliances with other types of occlusal splints
which includes, anterior bite plane, posterior bite
plane, pivoting appliance, soft/resilient appliance.
According to Dawson occlusal splints are classified
into permissive splints/muscle deprogrammer and
directive splints/non-permissive splints.9
Flat plane stabilization appliance
Flat stabilization appliance is otherwise known
as michigan splint, muscle relaxation appliance,
or gnathologicsplint. According to Manns et al
Ideally, when a stabilization appliance is placed
intraorally, it should produce minor alterations to
the maxillomandibular relationship other than that
produced by the thickness of the material. This
is the most commonly used appliance and when
properly fabricated it has the least potential to
cause adverse effects to the orofacial structures.8
A stabilization splint should provide an ideal
occlusion in both the static and dynamic situations.
Ash and Ramfjord describes the ideal occlusion :
The aim, therefore, a stabilization splint is to
provide the patient with a static occlusion in which the maximum number of occlusal contacts are
made simultaneously and with equal force between
the opposing teeth and the splint.6
Soft splints
The stabilization splint is well tolerated in the lower
arch than the upper arch as there is no satisfactory
way of thinning the margins of the splint while
keeping good retention. These appliances are
usually worn only at night and, if they are to be
successful, will produce some symptomatic relief
within 6 weeks. They should be replaced after
4 - 6 months as they lose their resilience with the
passage of time. The appliance is generally made
out of 2 mm polyvinyl. If a thinner splint is required,
overheat the material before vacuum forming, and
if a selectively thicker appliance is required (for
instance in a patient with an anterior open bite)
then layers can be added in particular areas (i.e.
anteriorly) to establish even occlusal contact.6
Posterior bite plane appliances
Posterior bite plane appliances (mandibular
orthopedic repositioning appliances) are generally
fabricated for the mandibular arch. This appliance
has claim to increase the overall physical strength
and also enhance athletic performance. This
appliance function by producing changes to the
vertical dimension and also alter the horizontal
maxillomandibular relationship. The major
concern regarding this appliance design is the
iatrogenically created posterior open bite, since
the occlusion occurs only on the posterior teeth,
allowing supraeruption of the unopposed anterior
teeth and/or intrusion of the opposing posterior
teeth
Traditional anterior bite plane
Palatal-coverage horseshoe shape appliance
with an occlusal platform mostly covering six
or eight maxillary anterior teeth (e.g., Hawley,
Sved, Shore). Clenching was prevented by this appliance by leaving posterior teeth not in
occlusion during closing or in parafunctional
activities. Supraeruption of posteriors is the major
drawback of this appliance which is extremely
unlikely if worn only at night.4
Mini anterior appliances
The concept of making this oral appliance was
first introduced in the mid 1900’s as the lucia jig
that engaged only a small number of maxillary
anterior teeth usually two-four incisors. Nociceptive
trigeminal inhibition tension suppression system,
the anterior midline point stop devices and the best
bite are certain variations that have appeared on
the market
Anterior repositioning appliance
The anterior repositioning appliance (also referred
to as an orthopedic repositioning appliance) is
primarily used for patients with disc displacement
with reduction. The appliance holds the mandible
in the anterior location to seat the condyle on to
the disc. It can be used as a temporary treatment
modality to gain symptomatic relief of painful
internal derangements, but not to “permanently”
recapture the TMJ disk.7
This type of appliance
should be used with caution, and just for short
periods of time, mainly recommended after
stabilization splint therapy.
Neuromuscular appliances
It has been claimed by the proponents of
neuromuscular dentistry that the use of jaw muscle
stimulators and jaw-tracking machines enables
them to produce an oral appliance at the ideal
vertical and horizontal position of the mandible
relative to the cranium.7
Pivot appliances
The device is fabricated using acrylic resin
material that covers the maxillary or mandibular arch with one posterior occlusal contact which is
placed as far posteriorly in each quadrant. These
appliance function by reducing intra-articular
pressure by condylar distraction. The pivoting
appliance was recommended for patients with
internal derangements or with osteoarthritis.
Unilateral pivot placed in the posterior region is
a modified version of this appliance. When the
mandible close on this pivot contralateral joint will
be loaded and slightly distract the ipsilateral joint.
Unfortunately, a potential adverse effect with the
use of this modified appliance may cause occlusal
changes as a posterior open bite in pivot area.4
Hydrostatic appliance
This appliance was designed by Lerman which was
primarily consisting of a bilateral water filled plastic
chamber and acrylic palatal plate. The patient’s
posterior teeth would occlude with these water
filled chambers. When a splint is inserted there is
an increase in occlusal vertical dimension beyond
the freeway space, allows a muscle relaxation to
function more efficiently during contact and be
less active during postural functions. This design
was later modified to become a tool that would
be retained under the upper lip, while the fluid
chambers might be positioned between maxillary
and mandibular posterior teeth.
Soft splints produced a slight increase in masseter
and temporalis muscle activity, but particularly the
masseter muscle. There is a shift in the balance
of activity away from the anterior temporalis
muscles with both splints, particularly at 10%
of the maximum clenching level. The temporalis
muscles shows a reduction in activity relative
to the masseter muscles may be a factor in the
therapeutic effect of both hard and soft splint,
although the relief is clearly greater with the hard
splint.3
For symptomatic patients associated with increased
nocturnal muscle activity, a soft occlusal splint is
likely to be contraindicated. A hard occlusal splint
appears a more likely successful treatment.10
Both the hard and soft occlusal appliances had
similar effects with no significant differences
regarding the pain intensity and muscle tenderness
reductions. However this should be taken with
caution because limited number of the included
publications that considered at a high risk of bias.2
Minimally invasive and conservative mode of
therapy is more beneficial for patients suffering
from temperomandibular disorders. Occlusal
splints are the best recommended treatment option
but there are numerous disagreements regarding
the durability and mechanism of action of these
appliances. Even though both hard and soft splins
can be used their efficiency is contradicted.7,9,11,16
Many studies have obtained recordings and
assessed the relationship between masseter and
anterior temporal muscles with TMDs. However,
Rugh and Solberg suggested that increasing
OVD would be responsible for the appearance
of muscle symptoms and that this increase would
lead to the worsening, rather than the amelioration,
of symptoms. It has been recommended that
stabilization splint therapy can significantly relieve
pain in patients with disc displacement without
reduction, in comparison with TENS.3,8
Pettengill et al did not find any difference between
HS and SS. Clinician should consider low-cost
therapies such as counselling and self-care and
be as much conservative as possible. The type of
splint design or material did not affect the results12
There is no significant differences in maximum
occlusal force with the use of canine protected hard
stabilization splint and use of a Bruxogard-soft
splint was accompanied by decrease in occlusal
force in patients with sleep bruxism3
Truelove et
al. (2006) did a randomized trial in which they
found that all patients shows significant results
irrespective of splint design14. According to okeson
Hard acrylic maxillary splints significantly reduce
nocturnal muscle activity in the majority of patients
while wearing the soft splint there is significant
increase in nocturnal muscle activity.9
In a nutshell it can be stated that both materials
has its own pros and cons so both hard or Soft
materials can be used for the fabrication of
occlusal splints. Hard acrylic resin splints which can be made from self-cured or heat cured acrylic
resin, forming hard and rigid occlusal surface
that resist wearing and lasts longer time, but
with long use of this splint a significant occlusal
changes can occur. Soft splints forms a flexible
occlusal surface that can be easily adjusted to
adequate contact pattern. However, this pliable
splints can exacerbate bruxism because the soft
material cannot be balanced leading to premature
posterior contacts.2
Many studies has proven that occlusal splint is
the most common and efficient treatment for TMD
patients with a success rate of 70-90 %. Based up
on much research, despite the many disagreements
regarding its efficiency, the both splints exhibit
successful outcome in patients who suffer from
functional disorders of the masticatory system.
Finally, the effect claimed by occlusal splints
remains to be confirmed, and more research is
needed to conduct further analysis.