
Introduction
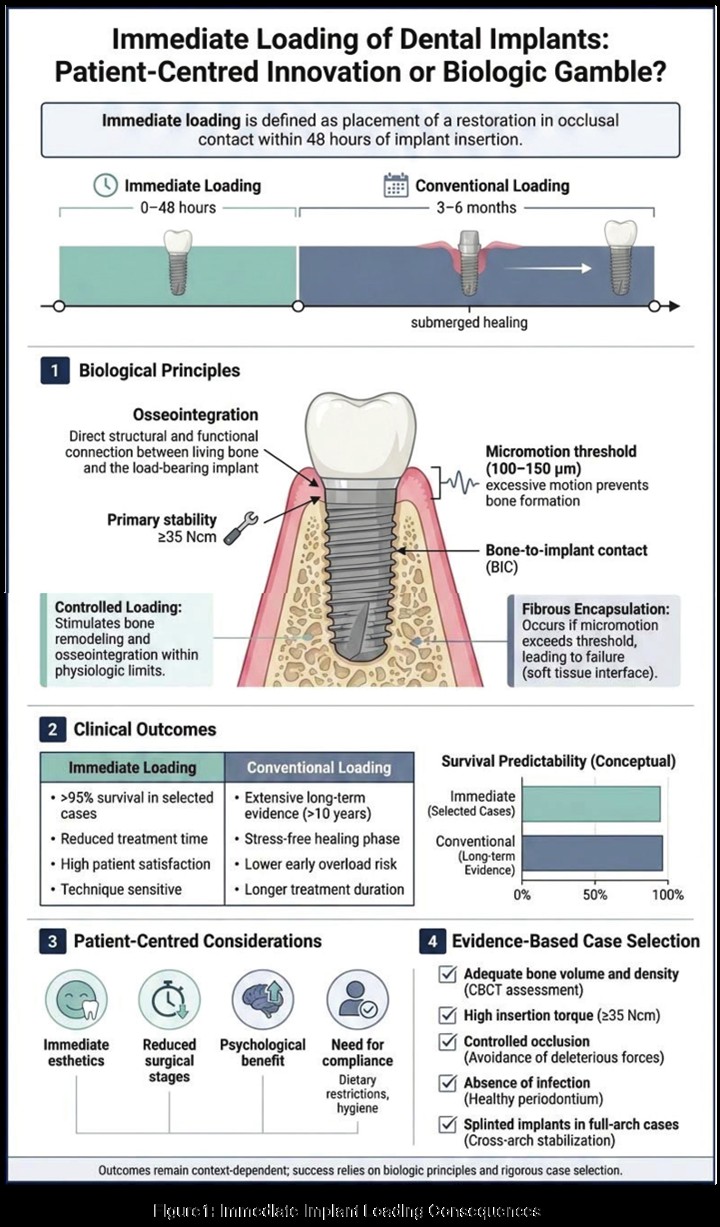
The concept of immediate loading of dental implants—defined
as the placement of a restoration in occlusal contact within 48
hours of implant insertion—has transformed implant dentistry
from a staged, months-long process into a potentially single
visit rehabilitation. Traditionally, osseointegration protocols
advocated by Brånemark required a submerged healing period
of 3–6 months to ensure predictable bone–implant contact1.
Immediate loading challenges this paradigm, positioning itself
as a patient-centred innovation. Yet critics question whether
bypassing conventional healing periods represents a biologic
gamble that may compromise long-term stability. A balanced
appraisal requires examination of clinical evidence, biologic
principles, and patient-centred outcomes.
Historical and Biological Foundations
Brånemark’s original protocol emphasised stress-free healing
to facilitate osseointegration, defined as a direct structural and
functional connection between bone and implant1. Albrektsson
et al. later identified critical determinants of implant success,
including biocompatibility, surgical technique, loading
conditions, and host factors2. Early micromotion beyond
100–150 µm during healing was associated with fibrous
encapsulation rather than bone formation, reinforcing the use
of delayed loading protocols3.
However, advances in implant surface technology and
macrodesign have altered the biologic landscape. Roughened
surfaces increase bone-to-implant contact and accelerate
osseointegration4. Proponents argue that when primary
stability exceeds 30–35 Ncm, insertion torque, and micromotion
are controlled, immediate loading does not inherently disrupt
bone healing5.
Here, there is agreement: both traditionalists and advocates
accept that primary stability and controlled occlusion are
prerequisites. Disagreement centres on whether these
conditions can be reliably achieved across diverse clinical
scenarios.
Clinical Outcomes: Comparable or
Compromised?
Systematic reviews offer valuable comparative insight. Esposito
et al., in a Cochrane review, reported no statistically significant
differences in implant survival between immediate and
conventional loading in carefully selected patients6. Similarly,
Papaspyridakos et al. reported survival rates exceeding 95%
in many immediate-loading studies7. These findings support
the view that immediate loading can be predictable under
controlled conditions.
Conversely, Lang et al. in an ITI consensus statement
emphasised that the evidence is strongest for immediate
loading in the edentulous mandible with splinted implants,
while data for single-tooth implants and posterior regions
are less robust8. Heterogeneity in study designs and follow
up durations complicates definitive conclusions. Critics note
that many trials are conducted in highly controlled settings
and involve experienced clinicians, potentially limiting
generalizability6,8.
Thus, while survival rates may be comparable in selected
cases, long-term data—particularly beyond 10 years—remain
less abundant than for conventional loading. The innovation
appears promising, but its predictability may be context
dependent (Figure 1)
Patient-Centered Advantages
From a patient perspective, immediate loading offers
substantial benefits. Reduced treatment time, fewer surgical
interventions, immediate esthetics, and psychological
satisfaction are frequently cited advantages5,7. In anterior
single-tooth replacements, immediate provisionalization
helps preserve soft-tissue contours and papillary architecture, enhancing esthetic outcomes9.
Moreover, immediate loading may reduce the need for
removable interim prostheses, improving quality of life during
healing7. Degidi et al. reported high patient satisfaction scores
associated with immediate functional loading protocols5.
However, the same patient-centred approach may introduce
risks if expectations exceed biologic limits. Immediate esthetics
can mask early implant instability, and patient compliance
becomes critical to avoid excessive occlusal forces. Thus, while
innovation enhances comfort and convenience, it demands
rigorous case selection and patient education.
Biologic Risks and Mechanical Challenges
The biologic gamble argument centres on micromotion and
overload. Misch highlighted that excessive early loading may
lead to crestal bone loss and implant failure, particularly in poor
quality bone10. Immediate loading in the posterior maxillae—
characterised by lower bone density—has demonstrated more
variable outcomes compared to the anterior mandible8,10.
Cochran et al. emphasised that while rough surfaces accelerate
osseointegration, they do not eliminate the biologic requirement
for stability during healing4. Furthermore, systemic factors such
as smoking, uncontrolled diabetes, and parafunctional habits
increase failure risk regardless of loading protocol2,8.
Mechanical complications also warrant consideration.
Papaspyridakos et al. reported slightly higher rates of prosthetic
complications in immediately loaded full-arch restorations,
including screw loosening and provisional fractures7. Although
these issues may not directly threaten osseointegration, they
add complexity and cost.
Hence, immediate loading is not inherently risky but becomes
so when biologic and mechanical principles are compromised.
It shifts the burden from time-dependent healing to technique
sensitive execution.
Evidence-Based Case Selection
Consensus guidelines underscore that immediate loading
is most predictable when several criteria are met: adequate
bone volume and density, high primary stability (≥35 Ncm),
absence of infection, controlled occlusion, and splinting in full
arch cases8. In contrast, delayed loading may be preferable
in grafted sites, poor bone quality, or when primary stability is
suboptimal.
This nuanced perspective reconciles innovation with biologic
caution. Immediate loading is neither universally superior nor
recklessly hazardous; its success hinges on adherence to strict
selection parameters.
Ethical and Economic Considerations
Economically, immediate loading may reduce overall treatment
time and associated costs, though it can require more complex
prosthetic planning. Ethically, clinicians must avoid marketing
driven enthusiasm that overshadows biologic realities. As
Esposito et al. caution, insufficiently powered studies and short
follow-ups can exaggerate perceived benefits6.
Thus, while patient-centred care supports minimising treatment
burden, evidence-based practice demands transparency
about risks and limitations.
Conclusion
Immediate loading of dental implants represents a significant
evolution in implantology, aligning with modern expectations
for efficiency and esthetics. Substantial evidence indicates
that, in carefully selected cases, survival rates are comparable
to conventional protocols. Technological advancements in
implant surfaces and surgical techniques have strengthened
its biologic foundation.
Nevertheless, immediate loading remains technique-sensitive
and context-dependent. Risks related to micromotion, bone
quality, systemic factors, and prosthetic complications persist.
The debate is less about innovation versus gamble and more
about indication versus indiscretion.
Ultimately, immediate loading is neither a universal solution
nor a reckless shortcut. It is a sophisticated protocol requiring
meticulous planning, sound biological understanding, and
individualised patient assessment. When applied judiciously, it
exemplifies patient-centred innovation. When indiscriminately
adopted, it risks becoming a biological gamble.
References