An 11-year-old female with Grade II right-sided microtia underwent stage II ear reconstruction and required postoperative support to prevent retro auricular sulcus obliteration and loss of auricular projection. Two weeks after surgery, considering the risk of early graft contracture, a temporary splint fabricated from impression compound was delivered as an interim measure to maintain ear elevation during the fabrication of a definitive appliance. After one week, a passive heat-cured polymethyl methacrylate (PMMA) acrylic splint was provided and secured to a spectacle frame tray using self cure acrylic resin to achieve stable retention and improved camouflage. The stepwise approach ensured continuous support of the elevated auricular framework while maintaining comfort and aesthetics. The patient was instructed to wear the splint daily. At 2-month follow-up, auricular projection was clinically maintained with no evidence of sulcus obliteration, skin irritation, pain, or appliance fracture. Patient compliance was excellent, and the spectacle-supported design enhanced social acceptability. This sequential splinting protocol represents a simple, cost-effective, and practical method for postoperative maintenance of ear projection in paediatric microtia reconstruction.
Key words: microtia, ear reconstruction, acrylic splint, spectacle-supported splint, auricular projection, postoperative management
Microtia is a congenital malformation of
the external ear characterized by partial or
complete absence of normal auricular structures.
Epidemiological studies report a prevalence
ranging between 0.8 and 4 per 10,000 live
births, with a higher incidence in males and
a predominance of unilateral involvement.¹
Autologous auricular reconstruction has evolved
significantly over decades, and multiple
classification systems—including those of Marx
and other surgical frameworks—aid in clinical
assessment and treatment planning.1,2
Autologous costal cartilage reconstruction
remains the gold standard for definitive auricular
rehabilitation.2,3 The Brent technique and its
subsequent refinement through the Nagata
method have established structured, multi-stage
protocols to achieve aesthetic and structural
restoration.3,4 Stage II reconstruction involves
elevation of the reconstructed auricle and
formation of a retroauricular sulcus to create an
appropriate cephaloauricular angle.5˒6 Despite
meticulous surgical execution, graft contracture
and scar maturation may compromise projection,
potentially leading to partial sulcus obliteration
or need for revision procedures.6˒7
To counteract these contractile forces,
postoperative splinting has been widely
advocated. Various techniques have been
described, including thermoplastic appliances,
customized splints, Foley catheter–based
devices, impression compound appliances, and
acrylic resin splints.8˒9˒10˒11 While these modalities
aim to preserve projection, concerns remain
regarding retention, structural rigidity, hygiene maintenance, and long-term compliance,
particularly in paediatric populations.8˒9
Therefore, development of a practical, stable,
and aesthetically acceptable splinting strategy
is clinically relevant.
This report presents a stepwise postoperative
splinting protocol employing an interim
impression compound splint followed by
a spectacle frame–supported heat-cured
polymethyl methacrylate splint for maintenance
of auricular projection following stage II microtia
reconstruction.
An 11-year-old female patient reported to the
Department of Prosthodontics for fabrication
of a postoperative splint following stage II
reconstruction of right-sided Grade II microtia.
The patient had undergone auricular elevation
with retroauricular sulcus formation two weeks
prior. There was no relevant medical history, no
syndromic association, and no history of hearing
aid use.
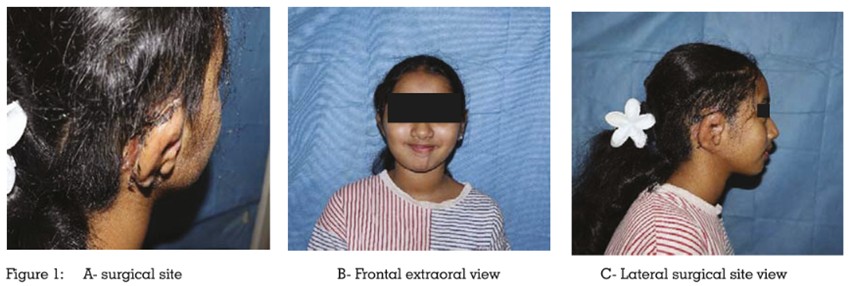
At presentation, the skin graft over the
postauricular region appeared healthy with
satisfactory healing (Figure 1). Auricular projection was clinically adequate; however,
slight tenderness was present on palpation.
Considering the risk of postoperative graft
contracture and potential sulcus obliteration
during scar maturation, preventive splint therapy
was planned.
A temporary splint was fabricated using regular
impression compound softened in a water bath
at 55–60°C. The softened material was directly
adapted over the retroauricular sulcus region
and contoured to engage the newly created
sulcus (Figure 2). The maximum thickness was
approximately 1.5 mm at its thickest portion.
Retention was achieved through mechanical
engagement of the sulcus and contour locking
without auxiliary support or adhesive. The splint was worn throughout the day for one week,
serving as an interim measure while the definitive
splint was being fabricated. No adjustments
were required during this period.
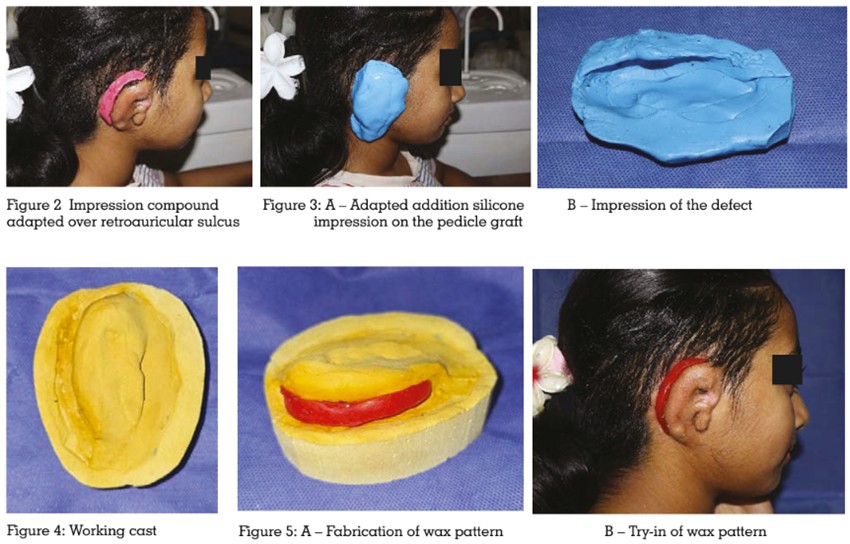
Impression and Cast Fabrication
At the first appointment for definitive splint
fabrication, an addition silicone putty impression
was made. The material was first adapted into
the sulcus region and subsequently extended
externally to cover the entire surgical site (Figure
3).
The impression was poured using Type III dental
stone to obtain a working cast (Figure 4).
Fabrication of Wax Pattern and Try-In
Modelling wax was adapted over the defect area
on the cast to fabricate a wax pattern. During
the second appointment, the wax pattern was
tried (Figure 5). The following parameters were
evaluated:
After confirmation of satisfactory fit and
projection, the wax pattern was processed.
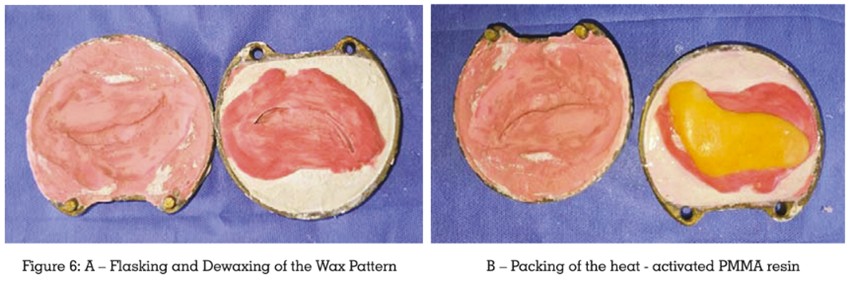
Laboratory Processing
The wax pattern was flasked using Type 3 dental
stoneand Type IV die stone, dewaxed, and
packed with heat-activated clear polymethyl
methacrylate (PMMA). Characterization was
achieved using intrinsic skin-tone pigments
blended with the acrylic resin. A commonly used heat-cure acrylic resin (DPI Heat Cure)
was utilized. The polymer-to-monomer ratio was
maintained at the manufacturer-recommended
3:1 ratio by volume. The material was processed
using a conventional compression moulding
technique and cured in a water bath at 74°C
for 8 hours following standard long curing
cycle protocols. After bench cooling to room
temperature, the prosthesis was deflasked,
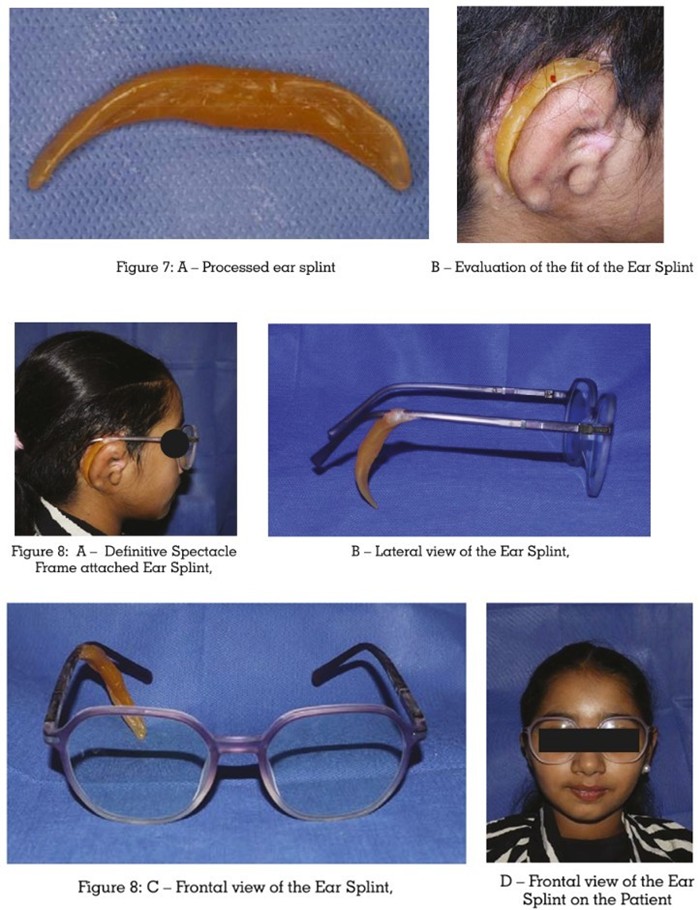
trimmed, and polished (Figure 6). The final
thickness was approximately 1.5 mm, and the
splint weighed approximately 25 grams.
Attachment of Spectacle Frame
During the third appointment, the processed
splint was evaluated for passive fit and projection
(Figure 7). The appliance was purely passive and
designed to engage the sulcus without exerting
active pressure. No relief was provided over the
grafted region to ensure adequate support and
maintenance of projection.
The patient’s own spectacle frame was used
for retention. The optimal attachment site was
identified and marked while the spectacles were
worn without the splint. The corresponding areas
on both the splint and spectacle frame were
roughened mechanically. Self-cure clear PMMA
resin was then applied to bond the splint to the spectacle tray while the patient maintained
proper positioning to ensure accurate alignment
(Figure 8). After polymerization, the attachment
site was trimmed and polished, and the
appliance was delivered.
Retention was achieved through sulcus
engagement and spectacle support. Stability
was ensured by maintaining proper positioning
during auto polymerizing resin setting.
Post-Delivery Instructions and Follow
Up
The patient was instructed to wear the appliance
during daytime hours for approximately 15
hours daily and remove it at night. The planned
duration of wear was four months until the third
stage surgical procedure.
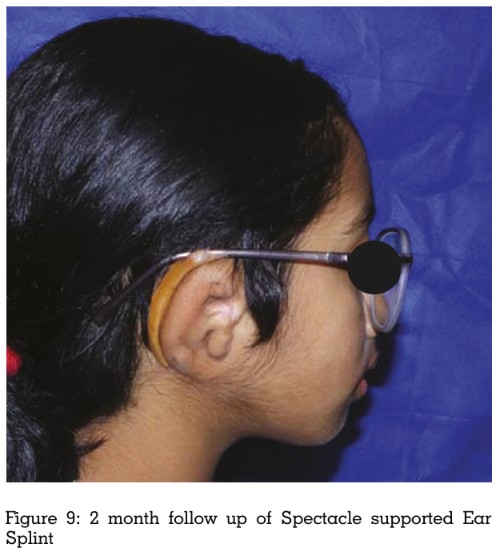
At 2-month follow-up, the patient continued to
wear the splint regularly (Figure 9). Auricular
projection was clinically maintained with no
evidence of sulcus obliteration. No erythema,
ulceration, fracture, loosening, or need for
relining was observed. Both patient and parent
reported satisfactory comfort and aesthetic
acceptance.
Comprehensive clinical and laboratory
documentation, including pre-splint, interim
splint, definitive splint, and follow-up images,
were recorded.
Maintenance of auricular projection following
stage II microtia reconstruction remains a critical
determinant of long-term aesthetic success.
Although cartilage framework support and
fascial coverage enhance stability, biological
remodelling processes such as scar contraction
remain unpredictable.5˒6 Even well-executed
reconstructions may demonstrate gradual
reduction in projection during maturation.⁷
Consequently, splint therapy functions as a
biomechanical continuation of the surgical
objective rather than merely an auxiliary
measure.
Multiple splinting modalities have been
described to maintain sulcus depth. Overview
literature emphasizes thermoplastic and
customized splints as commonly employed
approaches.8˒13 These devices are adaptable
but may lack sufficient rigidity for prolonged
structural support. Foley catheter–based splints
provide a cost-effective and relatively simple
method for maintaining sulcus patency.¹¹
However, their circular configuration primarily
offers tension-based support and may not
provide precise three-dimensional stabilization.
Impression compound has been reported
as an effective material for maintaining ear
elevation during early postoperative healing.¹⁰
Its thermoplastic adaptability allows intimate
sulcus engagement with minimal fabrication
complexity. However, its durability is limited
when prolonged support is required. In contrast,
acrylic resin splints offer superior dimensional
stability and resistance to deformation.9,14
Processed heat-cured PMMA allows controlled
rigidity, enabling sustained maintenance of
sulcus depth without repeated reshaping.
Nevertheless, careful adaptation is essential to
avoid excessive pressure over grafted tissues.
Recent advances include digitally fabricated
and three-dimensional printed splints.¹²
Randomized clinical evidence suggests
improved maintenance of cranioauricular
distance compared with conventional
thermoplastic appliances.¹² Stepwise workflow
protocols further emphasize reproducibility
and cost-effectiveness.¹⁴ However, specialized
equipment requirements and increased costs
may limit universal adoption.
Microtia reconstruction using autologous
cartilage
frameworks remains technically
demanding and
outcome-sensitive.2˒3˒4
Systematic reviews have reported measurable
complication rates, reinforcing the importance
of adjunctive postoperative support strategies.¹⁵
Integration of splint therapy into the reconstructive
algorithm may therefore enhance stability and
minimize projection relapse.
In the present case, a staged prosthodontic
approach combined early adaptable support
using impression compound with long-term
rigid stabilization through a heat-cured PMMA
splint. Spectacle-frame retention provided
discreet and socially acceptable stabilization,
improving compliance in a paediatric patient. At
two months, projection was maintained without
tissue irritation or mechanical complications,
supporting the clinical feasibility of this
sequential protocol.
The present report represents a single clinical
case with a relatively short follow-up duration
of two months. Objective measurements such
as cephaloauricular angle quantification or
standardized scar assessment scores were not
recorded, limiting quantitative comparison with
previously published data. Furthermore, the
absence of a control group precludes direct evaluation of superiority over other splinting
modalities. Long-term follow-up and prospective
comparative studies are necessary to validate the
durability and reproducibility of this sequential
splinting protocol.
Sequential postoperative splinting using interim
impression compound followed by a spectacle
supported heat-cure PMMA splint effectively
maintained auricular projection after stage
II
microtia reconstruction. This cost-effective,
patient-friendly approach provided stable
sulcus engagement, satisfactory aesthetics,
and good compliance, highlighting the value of
prosthodontic collaboration in interdisciplinary
microtia rehabilitation.