Introduction: Partial edentulism is a common dental
condition that affects oral function, aesthetics, and
quality of life. Understanding the pattern of tooth loss
helps in planning appropriate prosthodontic treatment
and implementing preventive strategies.
Aims and Objectives: To determine the occurrence
of various missing teeth patterns among the partial
edentulous patients residing in our area and
surrounding areas, who are undergoing treatment
for the replacement of missing teeth in the Department
of Prosthodontics, rural dental college in Tamil Nadu,
India.
Materials and Methods: Three hundred and sixty
persons aged between 13 and 87 years (115 males
and 145 females) who reported to the department of
prosthodontics between January 2020 and October
2025 were selected. Intraoral examination was done
visually, and results were recorded on specially
designed clinical examination forms.
Statistical Analysis & Results: Data were analysed
using the statistics SPSS 26.0 version (IBM India
Private Limited, Bangalore) to investigate the
relationship between quantitative variables. The
results showed that patients with Kennedy’s Class
III were the most prevalent group (54.2%). The most
common modification in all the groups was Class
III modification I (27.5%). It was also found that
Kennedy’s Class III was found more in the age
group of 31-40, with 55.1% in the maxillary arch
and 48.3% in the mandibular arch.
Conclusion: The findings of this study show that
Kennedy’s Class III was the most commonly
occurring and was found to be more predominant
in the younger population group.
Key words: partial edentulousness, Kennedy’s classification, missing tooth, gender, epidemiology.
Tooth loss has an impact on an individual’s
oral health-related quality of life at biologic,
psychological, and social levels. The prevalence
and extent of tooth loss have decreased
significantly in many countries during recent
decades. There still remains a significant
variation in tooth loss distribution. These
disparities may be attributed partly to the
increased availability and accessibility to oral
disease prevention and control programs,
as well as to increase in the awareness of the
importance of oral health. The study of trends
in tooth loss, comparing the rate of occurrence
between different populations, may provide
important information about risk factors for tooth
loss, potential changes in oral health status, and
possible causes of these changes.1
Tooth loss is identified by an edentulous space,
which is a gap in the dental arch normally
occupied by one tooth or more. It could be
partial or complete. A person may lack a few
teeth (partially edentulous) or all the teeth in
one or both upper and lower jaws (completely
edentulous) for various reasons. Studies have
observed that the major reason for tooth loss
across all ages was due to dental caries (36
68%), followed by periodontal disease (17-40%).2
A simple estimate of the percentage of partially
edentulous persons is a rough indication of the
frequency of dental diseases and the success or
failure of dental care. Observance of a pattern of
tooth loss determines the treatment requirement
among the population.
The design of the prosthesis depends on the
type of saddle area. A classification of partially
edentulous arches helps to identify the relation
of remaining teeth to edentulous ridges and
facilitates communication, discussion, and
comprehension of the suggested prosthetic
treatment among dentists, students, and technicians3,4. Kennedy’s classification, first
proposed by Dr Edward Kennedy in 1925, remains
the most widely used system for categorising
partial edentulism due to its simplicity and
clinical applicability.5
The pattern of tooth loss is a clear indicator of
levels of oral hygiene, dental health awareness,
the magnitude of dental problems, and the
management. Epidemiological studies related
to the status of a pattern of tooth loss are scarce
in India, especially in South India.5 Owing to the
large Indian population, a nationwide survey
cannot be done. However, the epidemiological
features of partial edentulousness of one
community can be assessed on the basis of a
cross-sectional study. The present study was
done in order to provide a complete reflection
of dental status and treatment needs, which
would be of valuable information to the National
Oral Health Planners for laying out strategies to
develop dental health care management in the
country.
Learning the truth that tooth loss and its effects
are so detrimental, our study aimed to find:
1. The incidence of Kennedy’s classification
among the partially edentulous subjects based
on gender ratio and age-wise distributions
2. Predominance of which type of Kennedy’s
classification among the patients attending
the selected dental clinics in our college for
replacement of their missing teeth.
This study was carried out from January 2025
to October 2025 among patients reporting to
the Department of Prosthodontics, rural dental
college in Tamil Nadu, for the replacement of
their missing teeth. A convenience sampling
technique was utilised for data collection, and
260 patients were selected. The sample size was calculated using the formula n = Z²pq/d² with
95% confidence interval, 5% margin of error, and
expected prevalence of 50%, yielding a minimum
required sample of 384, which was exceeded in
this study.
The inclusion criteria involved both genders,
aged between 13 years and 87 years, having
partially edentulous areas in either or both the
jaws. Completely edentulous patients and those
with only missing maxillary and mandibular third
molars were excluded from the study. Un-erupted
or congenitally missing teeth, root tips, and very
loose teeth that were indicated for extraction
were not included as remaining teeth and were
excluded from the study. The study population
was divided into two clusters, comprising 115
men and 145 women. The selected patients were
grouped according to their age (Table 1).
A pretested proforma was used, which includes
name, age, gender, and details of missing
permanent teeth. Clinical examination of each
patient was carried out after obtaining informed
consent, and intraoral examination was done
using a mouth mirror, probe in satisfactory
lighting, and direct visual examination. No
diagnostic aids like study models or radiographs
were used in this survey. The patterns of missing
teeth were identified according to Kennedy’s
classification
with Applegate’s rules for
application.
The number of teeth was defined as healthy,
carious or treated teeth (including crowned, inlay,
and abutment teeth for fixed partial prosthesis),
inclusive of completely erupted third molars. Data
analysis was carried out by using IBM SPSS 26.0
version, (IBM India Private Limited, Bangalore)
to estimate the percentage of predominantly
occurring Kennedy’s classification within the
genders and also according to age. The Pearson
Chi-square analysis test was conducted, and P<0.05 was considered to be statistically
significant. Ethical clearance was obtained
from the Institutional Ethics Committee before
commencement of the study.
Data were analysed by using IBM SPSS 26.0
version, the Pearson Chi-square analysis test
was conducted, and P < 0.05 was considered to
be statistically significant. The survey included
260 patients, of 115 (44.2%) male patients and
145 (55.8%) female patients aged between 13
and 87 years, having partially edentulous areas
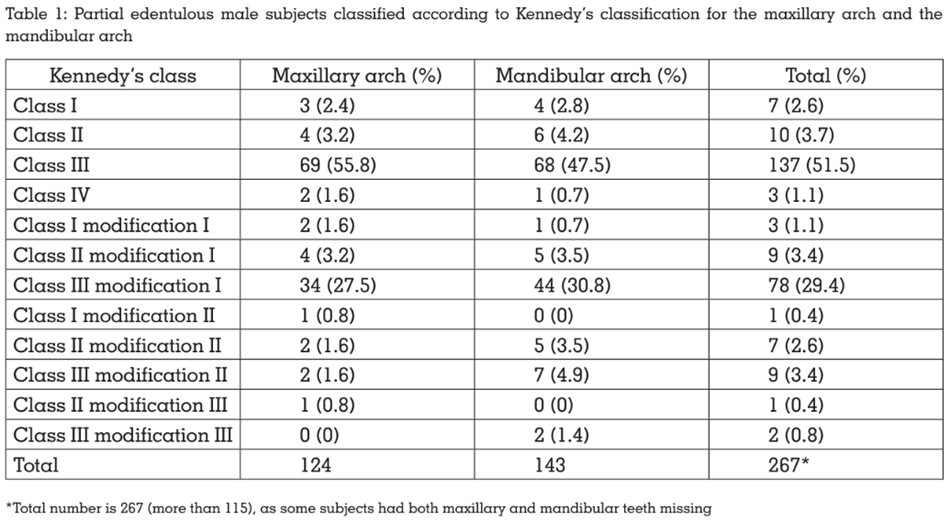
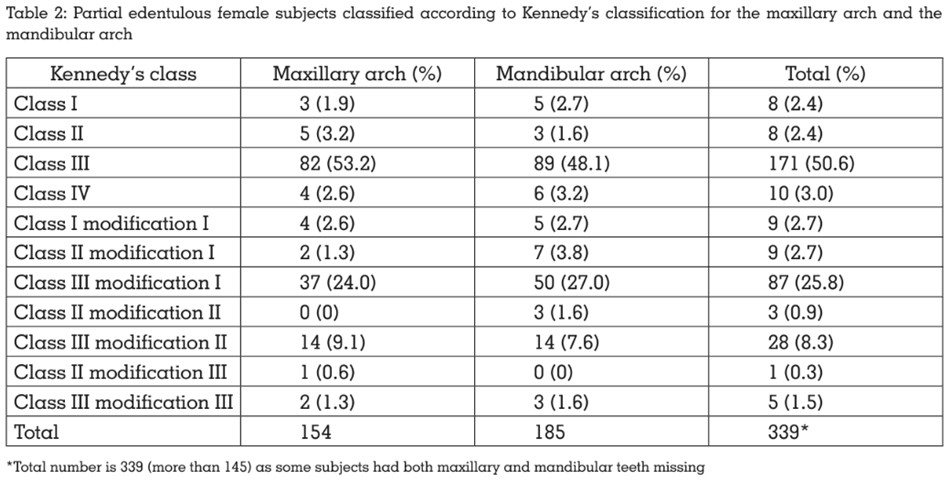
in either or both the jaws. Table 1 and Table 2
show the incidence of different patterns of partial
edentulism according to Kennedy’s classification
for males and females, respectively.
The results showed the occurrence of Class III
partial edentulism with 55.8% in the maxillary
and 47.5% in the mandibular arch for male
patients. Similarly, Class III type of partial
edentulism was also found in female patients,
with 53.2% in the maxillary and 48.1% in the
mandibular arch. This was followed by Class
III modification I in both the genders with an
average of 29.4% in male patients and 25.8% in
female patients.
Based on these results, patients with Kennedy’s
Class III were found to be the most prevalent
among both the genders (54.5%) in the maxillary
arch and (47.8%) in the mandibular arch, and
the most common modification was Class
III
modification I among both the genders
(26.8%) in the maxillary arch and (30.9%) in the
mandibular arch.
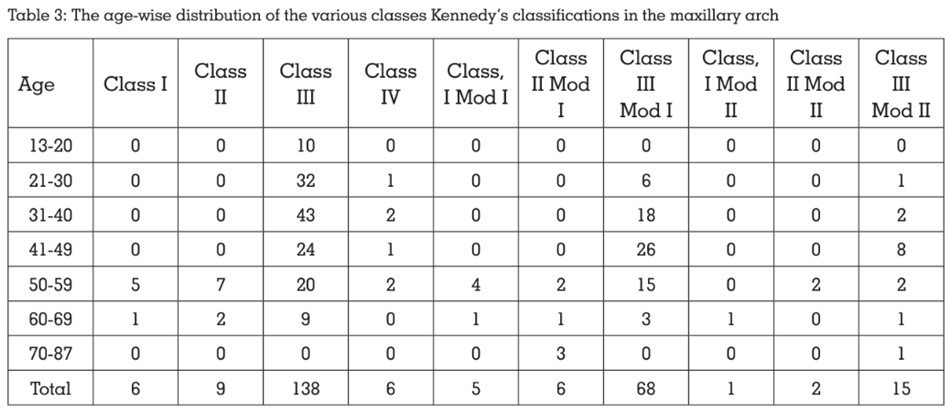
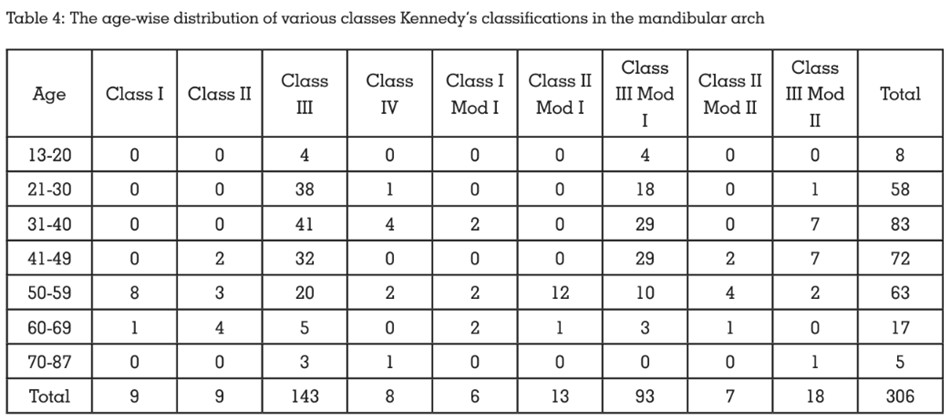
Tables 3 and 4 show Kennedy’s classification
for age-wise variation for the maxillary and
mandibular arch. The result showed Class III
predominance between 13 and 69 years in both
arches, while Class II modification I was found in the maxillary arch of age group 70-87 years. The
next predominant classification was Class III
modification I for all ages in both the arch except for the 50-59 years age group, which had Class
II modification I in the mandibular arch. Among
the different age groups, the predominance of Class III was found in the 31-40 years.
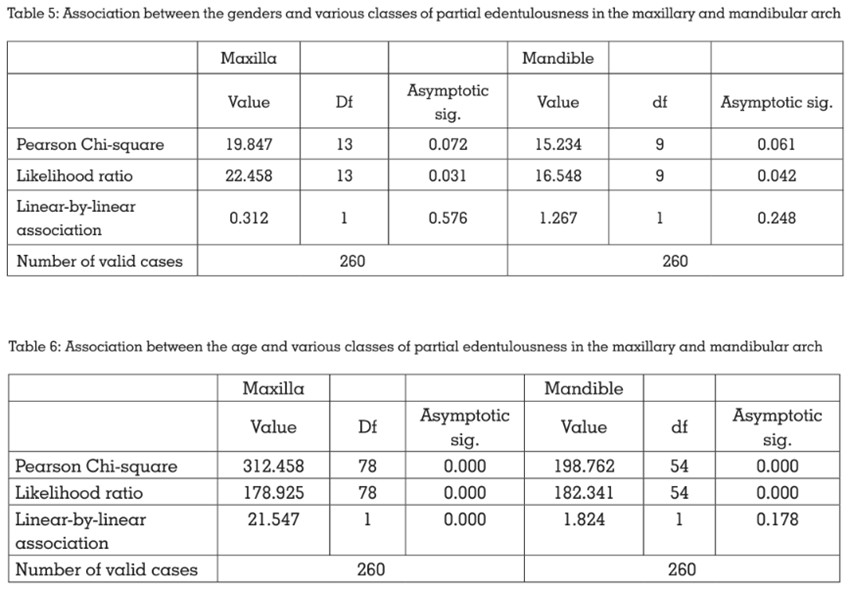
In this regard Chi-squared test was conducted
to analyze whether there is any correlation
when comparing the genders and also the age
with respect to Kennedy’s classifications in
the maxillary and the mandibular arch, and it
was found that there was no association when
compared between the male and female patients
for maxillary arch and mandibular arch (Table 5). It was also found that there is a significant
difference in the age-wise comparison of
the group in both the maxillary arch and the
mandibular arch (Table 6).
It is increasingly recognised that the impact of
the disease on quality of life should be taken
into account when assessing health status. It is likely that tooth loss, in most cases, being a
consequence of oral diseases, affects the oral
health-related quality of life (OHR QoL).6 In a
large Japanese study, Ide et al. found a strong
correlation between the number of missing
teeth and higher oral health impact profile
scores, suggesting impairment of OHR QoL.
Edentulous patients fall into a special category
among the various diseases of dental origin.
Tooth loss is the dental equivalent to mortality. A
simple estimation of the proportion of the partial
edentulous case is a rough indication of the
prevalence of dental diseases and the success
or failure of dental care.
Studies have reported that the prevalence of
partially edentulous adults ranges between 66.5% and 76.12% in various populations.7 In
the present study, more missing teeth were
seen in the female population (55.8%), which
is consistent with findings from some Indian
studies but contrary to studies from Romania,
where more missing teeth were found in the
male population.8,11
The results of the present study indicate that the
frequency of maxillary edentulism was higher
than that of mandibular edentulism among
the study population. Kennedy’s Class III was
found to be the most common pattern of partial
edentulism among all the age groups, both in the
maxillary arch and the mandibular arch, except
in the 70-87 years, in which Class II modification
I was predominant in the mandibular arch9,10.
The present study was partially in accordance
with Curtis et al.,10 wherein Kennedy’s Class III
was predominant only in the maxillary arches,
while in the mandibular arches, the most
prevalent pattern in the previous study was
Kennedy’s Class I. A major disparity between
the two studies is that of the age factor, as the
age group of Curtis’ study averaged 55 years,
whereas in this study, the average age of the
patients was approximately 38 years.
Al-Dwairi.,11, in a study, investigated the frequency
of different patterns of partial edentulism of 200
patients in Jordan and found that 150 had both
maxillary and mandibular partial edentulism.
In the present study, 9 different patterns
were identified, in which Kennedy Class III
pattern of edentulism was the most commonly
encountered in both the maxilla (54.5%) and
mandible (47.8%) arches, and Kennedy Class III
modification was the next most common from the
results. This study also correlates with the study
carried out on a Saudi population conducted
by Sadig and Idowu, examining 422 partially
dentate arches; Kennedy’s Class III was the
most commonly encountered pattern of partial
edentulism in both the upper and lower arches,
and Kennedy’s Class IV was the least common
pattern encountered.12
A comprehensive literature review by Jeyapalan
and Krishnan8,12,13. analysing studies over 24
years confirmed that Kennedy Class III remains
the most prevalent classification globally, with
consistent findings across diverse populations,
including Indian, Saudi Arabian, Jordanian,
and American populations. Recent studies from
Riyadh, Saudi Arabia, have also supported
these findings12,13,14.
The findings of the present study suggest that
a predominance of the Class III pattern of
partial edentulism may be due to the fact that
a higher frequency of younger age groups was encountered, whereas a higher frequency of the
older population was seen in previous studies15,16.
The present study also shows increased
awareness among the younger population, with
a large number of younger groups reporting to
the prosthodontics department for replacing the
missing tooth. The higher frequency of partial
edentulism in these younger age group patients,
as depicted by the results, might pertain to their
low socioeconomic status; poor oral hygiene and
less conservative treatment approach, relating
to lack of time, leading to early tooth loss17,18.
The data obtained from the present study on
the frequency and distribution of tooth loss are
very important to provide practitioners with the
information needed to address various factors
implicated in tooth loss, to reduce its mortality
and also to educate and to motivate patients on
the importance of saving teeth. At the national
level, these data also suggest that preventive
strategies aimed at reducing tooth loss need
to be reinforced. Petersen and Yamamoto.,9
reported that oral diseases and chronic diseases
share common risk factors. Hence, the National
Health Programs should incorporate disease
prevention and health promotion measures using
a common risk factor approach in combination
with the strategies to prevent tooth loss, which
need urgent attention by the policy makers for
older people.
The present epidemiological study reported
the prevalence of missing teeth in different age
groups and genders, which showed the existence
of Class III followed by Class III modification I,
which were predominant among the younger
population of 31-40 years, while in the geriatric
population between 70-87 years, Class II
modification I was present. Comprehensive
information on tooth loss is required to form a
generalised database for the partial edentulism patterns, which will help us in the identification of
the causes of such tooth loss and its prevention.
There are possible limitations in this study, as
the following factors were not evaluated. The
cause of the tooth loss, the literacy level, and
the socioeconomic status were not evaluated
to identify the reason for tooth loss, nor were
chronology for tooth loss, and radiographs
were not used to identify congenitally missing
and impacted teeth. Future studies with larger
sample sizes and inclusion of these variables
would provide more comprehensive insights into
the epidemiology of partial edentulism in this
region.