Accurate centric relation (CR) recording is crucial for successful complete denture fabrication. With the digitalization of denture fabrication, it is essential to retain the accuracy while improving efficiency. Yet, existing digital workflows often require repeated design and printing of tracer components for each patient. This study presents a hybrid technique which is an approach to enhance Gothic arch tracing using a 3D-printed CAD-based tracer attachment of a conventional intraoral tracer. This digital workflow utilizes intraoral scanning data to design custom denture base with tracing attachments, which is 3D- printed and can be attached to the conventional intraoral tracer, minimizing 3D printing and simplifying the process. Despite technological advancements, current digital methods remain limited by cost and adaptability. This technique bridges conventional and digital workflows, reducing chairside time while maintaining precise, repeatable CR records.
Key words: digital denture, centric relation recording, gothic arch tracing
Traditionally, conventional complete dentures
(CD) were the standard treatment for an edentulous condition. CD have provided reliable
rehabilitation for decades; however, the process
is time-consuming and requires multiple clinical
appointments, extensive laboratory procedures,
and physical storage of records.1 Digital dentures
were introduced in 1994, and their protocols
continue to evolve with advances in scanning,
design, and manufacturing technologies.2 Centric
relation (CR) and vertical dimension of occlusion
(VDO) are critical determinants of successful
complete denture outcomes. According to the
Glossary of Prosthodontic Terms, CR is the
maxillomandibular relationship, independent
of
tooth contact, in which the condyles
articulate with the thinnest avascular portion
of their respective discs with the complex in an
anterior-superior position against the slopes of
the articular eminences; this position is clinically
discernible when the mandible is directed
superiorly and anteriorly.3 In both conventional
and digital workflow, it is essential to record CR
in a repeatable, accurate, and verifiable manner
for functionally stable complete denture.
Among the various methods of recording CR,
Gothic arch tracing stands out for its clinical
reliability, as it produces a visible arrow-point tracing that indicates the apex of mandibular
movement and simultaneously records
centric, lateral, and protrusive movements.4
Conventional workflows are now gradually
transitioning to digital methodologies. It
incorporates, intraoral scanning, 3-Dimensional
(3D) printing, and Computer Aided Designing/
Computer Aided Milling (CAD/CAM) systems.
It can be complemented by optical jaw-tracking
systems, that digitally record mandibular motion
and maxillomandibular relationships.5 However,
these innovations still face challenges, including
procedural complexity, cost, and the need
for digital proficiency. The current digital CR
recording methods lack universally validated,
cost-efficient, and adaptable protocols for
routine clinical use.
Present article introduces a hybrid technique
that utilizes a reusable Standard Tessellation
language (STL) file of the tracer attachment
combined with a conventional intraoral Gothic
arch tracer. The method integrates intraoral
scan data to design custom denture bases
with standard tracer attachments, minimizing
repeated printing and streamlining the digital
workflow. By combining the clinical reliability
of conventional Gothic arch tracing with the
efficiencies of digital design, the limitations of existing systems are addressed. This technique
balances clinical reliability with digital efficiency.
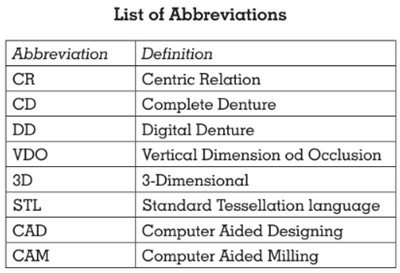
Step 1: Maxillary and mandibular edentulous
arches are scanned using an intraoral scanner
(Medit i500, Medit Corp., South Korea) to obtain
baseline digital casts (Fig. 1).
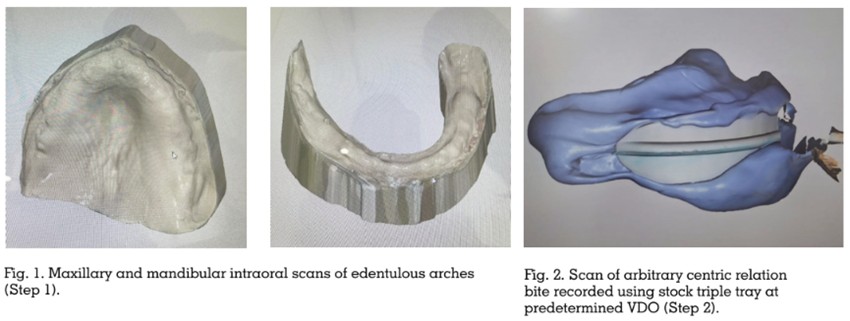
Step 2: Putty-consistency elastomeric impression
material (3M Express XT VPS Impression
Material, 3M ESPE, Germany) is loaded on
a triple tray to record an arbitrary CR at a
predetermined VDO, and this record is scanned
to digitally orient the maxillary and mandibular
arches in arbitrary centric relation (Fig. 2).
Step 3: The aligned scan data are imported
into CAD software (Exocad DentalCAD, Exocad
GmbH, Germany) to design custom trays with
occlusal rims for both arches.
Step 4: The tracer attachment of the conventional
intraoral Gothic arch tracer (Bio Tracer FB, Bio-
Art, Brazil) is scanned to obtain an STL file, which
is stored for repeated use in multiple cases.
Step 5: Custom maxillary and mandibular
denture bases with occlusal rims are digitally
designed in the CAD software, using the oriented
digital casts as the reference.
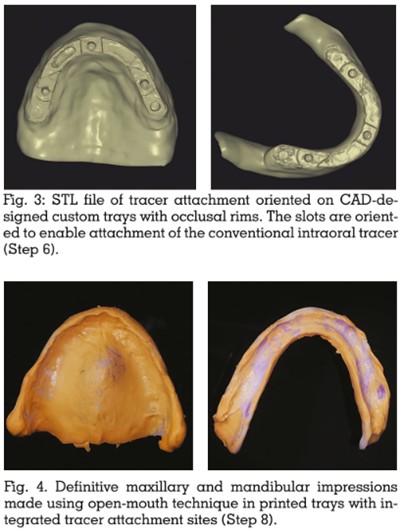
Step 6: Thus, the STL file of the tracer attachment
(approximately 5.0±0.1 mm thickness) is
positioned on the maxillary and mandibular
occlusal rims in the design software to create
a standardized site for attachment of the
conventional intraoral tracer (Fig. 3). The
position of the tracer is verified by digitally
superimposing it over the attachment.
Step 7: The denture bases with integrated tray
and tracer-attachment design are 3D printed
using a resin printer (AccuFab-L4K, Shining
3D, China) with a 50-μm layer thickness. These
printed bases serve as special trays for definitive
impression making and for supporting the
intraoral tracer during CR recording.
Step 8: The printed maxillary and mandibular
trays (each with integrated tracer attachment
sites) are tried intraorally and adjusted for fit
as needed. A definitive impression is made using the openmouth technique with light
body elastomeric impression material (3M
Express™ XT Light Body, 3M ESPE, Germany)
(Fig. 4). The final impression shall be done
after border molding with heavy-body material,
when required. The trays now contain definitive
impressions, accurately capturing intraoral
features for subsequent CR recording.
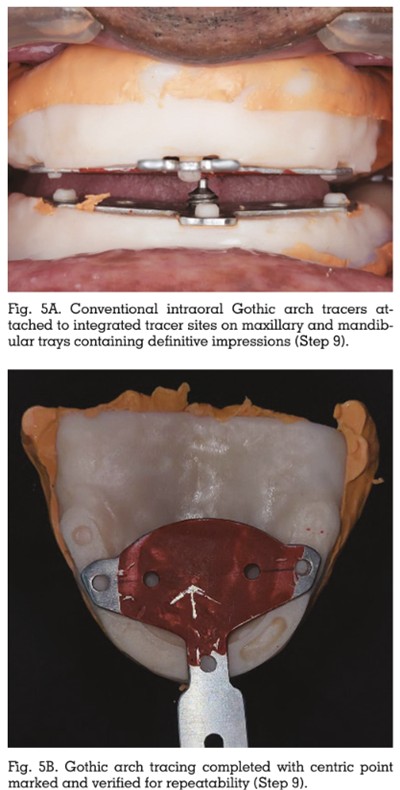
Step 9: The pre-determined VDO is verified by
placing the metal bite rims provided with the
Bio Tracer FB (Bio-Art, Brazil) over the tracer
attachment sites, along with verification through
phonetics. With the definitive impressions
intact in both maxillary and mandibular trays,
conventional intraoral Gothic arch tracers are
attached to the integrated tracer attachment
sites. The trays are seated intraorally (Fig. 5A).
The patient is guided to perform protrusive
and lateral movements to obtain a Gothic arch
tracing, and the centric point is marked and
verified for repeatability (Fig. 5B).
Step 10: After recording CR, the maxillary
and mandibular printed bases with definitive
impressions and tracer components are scanned
using a laboratory scanner. The definitive
impression-based casts and the verified CR
position are transferred to a compatible virtual
articulator (Stratos 200, Ivoclar, Liechtenstein)
within the CAD software to design the definitive
complete dentures according to the recorded
mandibular dynamics.
CR is crucial for complete denture treatment
because it provides a stable, repeatable
reference position for developing occlusion in
patients who lack proprioceptive guidance from
natural teeth.6 The methods for recording CR
have evolved over time with changes in biologic
understanding and technological advances, yet
accurate and reproducible registration remains
a key determinant of denture success.7
The fundamental concepts employed in this
proposed workflow is similar to established BPS
principles. The maxillary and mandibular arches
are scanned and oriented using an arbitrary
centric record at a predetermined VDO, and the
data are stored digitally for easy communication
and duplication or modification of dentures when required in the future.8 A reusable STL
file of the tracer attachment for a conventional
intraoral Gothic arch tracer is incorporated into
the design, allowing precise and cost-effective
CR recording while reducing repetitive design
and printing of tracer components. By combining
definitive impression making and CR recording
within the same appointment, the approach
reduces the number of visits and laboratory
steps, which can benefit patients with limited
access or mobility.8 The definitive impression
captures areas that may be difficult to record
accurately with intraoral scanning alone, and
the conventional intraoral tracer is then used
to record centric and eccentric mandibular
movements, with the Gothic arch tracing
providing visual confirmation and repeatability
of the centric position.
Optical jaw-tracking systems record mandibular
motion in three dimensions and transfer it
directly to virtual articulators.9 These systems
provide detailed dynamic records but require
specialized equipment, software integration,
and calibration. This increases cost and
technique sensitivity. In contrast, this hybrid
technique uses widely available CAD/CAM and
3D printing with a familiar Gothic arch tracer
workflow. This makes it more accessible for
clinicians transitioning to digital dentures.
Other digital techniques custom-print new
trays and tracing assemblies (tenon-and
mortise joints) for each patient, following BPS
concepts.10 These workflows require multiple
printed components and additional steps for jaw
relation transfer. This technique uses reusable
STL tracer attachment integrated into the denture
base design. This eliminates repeated printing
of tracer parts. It saves time and materials while
maintaining visual CR verification through
the Gothic arch tracing, making it suitable for
resource-limited settings. The novelty of the technique lies in its digital implementation and
workflow optimization.
A key limitation of the present technique is the
use of a model resin that is not certified as a
long-term intraoral biocompatible material. In
this report, the resin was used only for short-term
intraoral procedures (definitive impression
making and CR tracing) and no adverse
reactions were observed, but this still represents
a limitation. Future work should validate
dedicated biocompatible tray resins such as
Arma Dental 3D Printing Resin (Arma Dental
Production Systems, Turkey) or Formlabs Custom
Tray Resin (Formlabs Inc., USA) as alternatives
to model resins.11
Additionally, successful application of the
method requires familiarity with digital design,
careful calibration of the tracer attachment to
avoid errors in vertical dimension, and validation
of the workflow across larger samples and
different operators. Future work could integrate
intraoral digital CR recording withdynamic
mandibular tracking technologies like Metismile
MR (Shining 3D, China). Further studies
comparing this hybrid approach with fully digital
jaw-tracking systems and other digital denture
protocols could help refine indications, quantify
accuracy, and standardize its use in routine
clinical practice.
This hybrid technique integrates conventional
Gothic arch tracing with digital denture design
for accurate CR recording. The reusable STL
file of the tracer attachment eliminates printing
multiple components while maintaining clinical
reliability. It provides a cost-effective solution for
digital complete denture workflows in resource
limited settings.