Hand defects significantly impact daily activities and psychological well-being. Prosthetic rehabilitation restores both function and confidence. This report describes the fabrication of a conventional interim hand prosthesis for a 65-year-old male patient with partial hand loss following traumatic amputation. Using traditional impression and acrylic molding techniques, a cost-effective prosthesis was fabricated, offering satisfactory aesthetics and psychological comfort. The described method remains a practical solution in resource-limited settings lacking access to advanced prosthetic facilities.
Key words: hand prosthesis; interim prosthesis; psychosocial rehabilitation
The loss of a hand due to trauma, congenital
absence, or medical conditions can have
a profound effect on both function and
psychological
well-being.1,2,3
Prosthetic rehabilitation restores aesthetics, functionality,
and quality of life.2-4 While definitive prostheses,
such
as
silicone, implant-retained, and
myoelectric designs, offer long-term solutions,
an interim acrylic hand prosthesis serves as a
crucial transitional phase in rehabilitation.1,5
Interim prostheses help patients to adapt both
physically and psychologically to prosthetic use,
which is designed to maintain tissue contour
and provide a transition for patients awaiting
definitive prosthetic fitting.6 Acrylic resins, widely
used in dental and maxillofacial prosthetics, are
preferred for interim hand prostheses due to their
ease of fabrication, cost-effectiveness, and ability
to provide a satisfactory aesthetic outcome.
Compared to silicone, implant-supported and
myoelectric options, acrylic prostheses offer a
practical and affordable solution for short-term
rehabilitation needs.7 This case report describes
a cost-effective and novel technique for the
rehabilitation of a partially amputated hand with
a custom-designed acrylic hand prosthesis by using cold-cure acrylic with acceptable aesthetic
results.
A 65-year-old male reported to the Department
of Prosthodontics with a history of right-hand
traumatic amputation sustained 20 years
ago. The amputation resulted in the loss of all
fingers and a significant portion of the upper
palm, except for the thumb. The patient had
been using a preformed hand prosthesis for
two decades, which exhibited severe wear
and deterioration. He expressed a desire for a
replacement but cited financial limitations in
acquiring an advanced prosthesis immediately.
After a thorough discussion of available options,
the patient elected to receive an interim acrylic
resin prosthesis, with the intention of fabricating
a definitive prosthesis at a later stage. The
patient was informed about the functional and
aesthetic limitations of the prosthesis.1,5,7-11
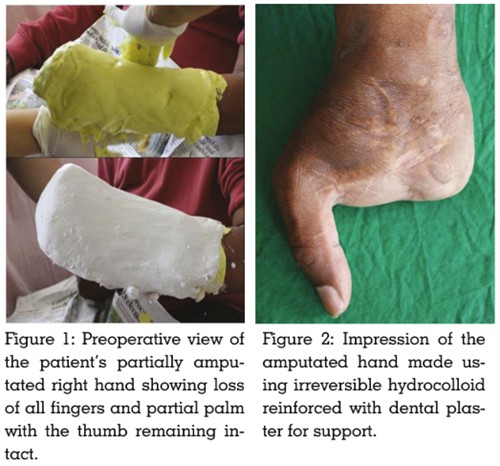
The impression of the amputated hand was
made with irreversible hydrocolloid impression material (Algitex; DPI), after coating the skin
with petroleum jelly. For reinforcement, Type II
dental plaster (MAARC Dental Plaster of Paris;
Aarkay Group) was added as a supportive layer.
Once set, the patient carefully removed his hand
from the mold. The impression was then poured
with Type III dental stone (Gold Stone; Asian
Chemicals)using a vibrator to prevent voids,
resulting in a positive replica.1,5,7-11
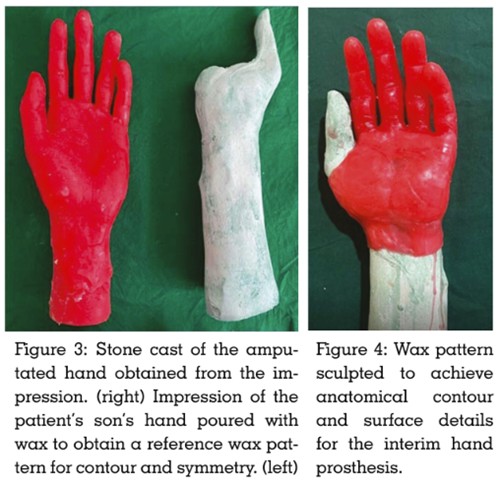
To achieve optimal anatomical accuracy, an
impression of the patient’s son’s hand was also
made and poured with Type III dental stone.
This served as a reference model for wax pattern
fabrication, aiding in contour development and
symmetry with the contralateral hand.1,5,7-11
The wax pattern was sculpted using additional
impressions, incorporating fine details such as
minor creases and natural depressions. The
length, shape, and fit of the wax pattern were
verified for harmony with the adjacent hand, and
necessary modifications were made to refine
adaptation and aesthetics.1,5,7-11
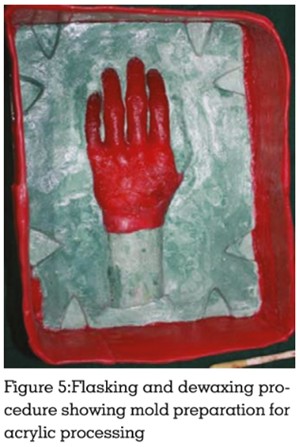
The wax pattern was invested in a custom
made box to facilitate flasking. The model
was flasked using Type III dental stone, while
Type IV die stone (Gyp Rock Die Stone; Rajkot
Dental Depot) was used in the wax-up area to
enhance surface hardness. Standard de-waxing
procedures were followed. Internal staining of
the dorsal and ventral surfaces was performed
separately to match the patient’s skin tone. A
separating medium was applied before acrylic
processing.1,5,7
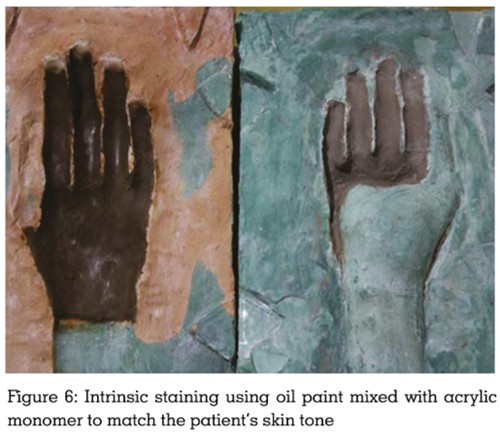
A mixture of oil paint (Camel Artist Oil Colours;
Kokuyo Camlin) and self-cure acrylic monomer
was prepared to match the patient’s complexion.
Clear cold-cure acrylic powder (DPI Cold Cure
Acrylic; DPI) was incorporated with the pigmented
monomer to form a homogeneous mix. The nail
portion was fabricated using a combination of pink and clear auto-polymerizing resin to match
the adjacent fingernails. The mold was packed
with the prepared acrylic, and standard flasking
procedures were followed.1,5,7
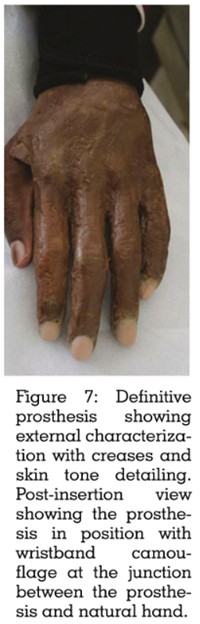
The flask was carefully opened, and the
prosthesis was retrieved. Finishing and polishing
were performed, and external characterizations,
such as fine lines and creases, were added to
enhance realism.
The patient was recalled for a trial fit, and
the prosthesis was delivered after final
adjustments. Chairside external staining using
oil paint enhancedcolour precision. The patient
was provided with detailed instructions on
maintenance, including cleaning with mild soap
and lukewarm water and avoiding exposure
to strong solvents. Regular follow-ups were scheduled to assess the patient’s comfort, fit,
and satisfaction.1
The patient was delighted with the function
and aesthetics of the interim prosthesis. The
prosthesis successfully restored a degree of
hand functionality while improving the patient’s
confidence and social interactions.1
The rehabilitation of hand amputees has been
explored extensively, with various prosthetic
options available, including silicone, myoelectric,
and acrylic resin prostheses. Studies have shown
that silicone hand prostheses provide superior
aesthetics, flexibility, and durability compared
to acrylic alternatives.2 However, their high cost
often limits accessibility, particularly in resource
limited settings.12 Myoelectric prostheses offer
functional benefits through electromyographic
(EMG) control, but they are expensive and require
periodic maintenance.13 Acrylic resin prostheses,
as demonstrated in this case, provide a cost
effective solution with acceptable aesthetics and
function. Similar findings have been reported in
cases of acrylic finger prostheses, where heat
cured acrylic material provided an affordable
and aesthetically acceptable alternative.9,14
This case underscores the importance of
prosthetic rehabilitation, particularly in
financially
constrained individuals, where
interim solutions like acrylic resin prostheses
provide temporary yet meaningful benefits. The
patient in this report experienced improved self
confidence and social integration, aligning with
similar outcomes reported in the literature.15
Fabricating an acrylic resin prosthesis
presents several challenges. The impression
making stage requires precise techniques to
capture anatomical details for optimal fit and
comfort.16 Additionally, achieving a lifelike colour match through intrinsic and extrinsic staining is
crucial but challenging, as acrylic materials lack
the translucency of silicone.17 Another significant
limitation of acrylic resin prostheses is their
lack of flexibility, which reduces comfort and
adaptability during prolonged use. Furthermore,
these prostheses are less durable and require
periodic maintenance or replacement, making
them less ideal for long-term wear.18
The longevity of an acrylic resin prosthesis
depends on usage, maintenance, and material
properties. Literature suggests that acrylic
hand prostheses typically last 2–5 years before
requiring replacement. To improve outcomes,
advancements in material science, such
as incorporating flexible acrylics or hybrid
materials, may enhance durability and comfort.
Additionally, periodic follow-ups are essential
to assess wear and tear and explore transitions
to more advanced prosthetic solutions, such as
silicone or myoelectric prostheses.
Fabricating large hand prostheses poses
additional challenges. One of the primary
difficulties encountered in this case was the
inability to use a regular flask for flasking
and packing due to the prosthesis’s size. This
limitation made the heat-cure acrylic option
impractical. The patient was informed about
the functional and aesthetic limitations of self
cure acrylic material, and with his consent, it
was decided to proceed with a self-cure acrylic
prosthesis. While self-cure acrylic provides
a cost-effective alternative, its mechanical
properties are inferior to heat-cured acrylic in
terms of strength and durability.16
Additionally, during the fit-in stage, a noticeable
transition was observed between the prosthesis
and the patient’s natural hand. To address this
aesthetic concern, a wristband was used to
effectively camouflage the junction, ensuring a more natural appearance and improving patient
satisfaction.
A quick, convenient, and affordable method of
making a hand prosthesis has been presented.
Self-cure acrylic is clearly not the best material
for a hand prosthesis, but considering the
financial constraints of the patient and the
ease of fabrication, this material was chosen to
fabricate the interim hand prosthesis. The glove
like prosthesis is easy to wear and remove. The
patient was comfortable and satisfied with the fit
and aesthetics of the prosthesis.
DECLARATION OF GENERATIVE AI AND
AI-ASSISTED TECHNOLOGIES IN THE
WRITING PROCESS
During the preparation of this work, the author(s)
used ChatGPT and Claude to summarize a few
portions of the original written draft of the case
report. All content generated with the assistance
of these tools was reviewed and edited by the
authors to ensure accuracy with the scholarly
standard of the work. The authors take full
responsibility for the content of the manuscript.