Dental implants have become an integral part of prosthetic dentistry, offering both functional and aesthetic solutions to edentulous patients. However, implant thread exposure can compromise implant stability and esthetics, potentially leading to peri implant complications. Various management strategies, including surgical and non-surgical approaches, have been explored to address this issue. This case report presents the use of implantoplasty combined with free gingival grafting as a successful approach for managing implant thread exposure.
Key words: thread exposure, implantoplasty, dental implants
Dental implants have provided documented
aesthetic and functional outcomes with long
term success rates.1 Implant thread exposure
represents a significant complication that can
jeopardize the structural integrity and longevity
of dental implants.2 Etiology of implant thread exposure is multifactorial and complex with
several contributing factors like mechanical
overloading, peri-implant infections, surgical
factors like improper implant positioning,
anatomical limitations, soft tissue factors like
insufficient keratinized tissue width and frenal
tension, physiological bone remodelling that
leads to marginal recession over time, certain
implant designs and surface characteristics
which could also contribute to increased thread
exposure risk.1-5 Management strategies for
implant thread exposure varies significantly,
encompassing both surgical and non-surgical
approaches based on the severity of the
condition and the underlying cause. Soft
tissue augmentation techniques, like flap
advancement and free gingival grafts (FGG),
have been shown to effectively increase the
keratinized tissue width while simultaneously
reducing clinical parameters associated with
inflammation.5,6 In cases involving significant
bone loss, guided bone regeneration (GBR) with autogenous grafts, especially cortical block
grafts from the mandibular symphysis, along
with xenografts and allografts, can help restore
the compromised osseous architecture.2,6 Non
surgical approaches of regular professional
cleaning with antimicrobial treatment, splinting
of implants, and use of angled abutments to
improve implant positioning can aid in controlling
infection and slowing disease progression.3,6
Implantoplasty has been proposed as an
adjunctive therapy for the management of
implant thread exposure.7-9 The procedure
involves mechanical modification of exposed
implant surfaces using diamond burs to remove irregularities and create a smooth and polished
plaque-resistant surface with a goal of restoring
the physiologic biological width.7,8
This case report addresses the successful
management of implant thread exposure
after stage-one implant placement through a
conservative and effective treatment approach
of implantoplasty and free gingival grafting.
A 22-year-old male patient visited the department
for the replacement of missing teeth and the
restoration of fractured teeth (Fig. 1A). The patient
had no relevant medical history but mentioned about implant placement four months prior.
Previous dental records revealed a history of
facial trauma sustained a year ago with multiple
dental injuries and no reported incident of facial
bone fracture. His records also indicated Ellis
Class III fracture of teeth #12 and #34, which
were endodontically treated; an Ellis Class VIII
fracture of tooth #23 that was extracted, followed
by an immediate implant placement (GMI;
3.75×13 mm); and an Ellis Class V fractures of
teeth #11, #21, #22, #32, and #33 with implants
placed in region #11 (GMI; 3.30×13 mm), #21
(GMI; 3.75×13 mm), and #33 (GMI; 3.75×13
mm) (Fig. 1A, 1B).

Intraoral examination revealed all implants to
be adequately covered with soft tissue except the
one located in the 33 region that showed thread
exposure (Fig. 1B) and a lack of attached gingiva.
The limited width of the attached gingiva, along
with the tractional pull of the lower lip, could
potentially worsen thread exposure. However,
the patient was not willing for any major
surgical interventions for the management of thread exposure and expressed a preference for
expedited prosthesis placement.8
At the second-stage surgery, exposure of
all the other implants confirmed successful
osseointegration without mobility. Healing
abutments were placed on all the implants. Since
the implant in 33 region with thread exposure did
not show any mobility, implantoplasty combined
with FGG was planned to increase the width
of keratinized attached gingiva and minimize
the severity of thread exposure.8,9 Elevation of
a full-thickness mucoperiosteal flap around
the affected implant revealed an advanced
buccal bone loss exposing around nine implant
threads (Fig. 2A). After thorough debridement
and removal of granulation tissues with hand
instruments, implantoplasty was performed
using a high-speed handpiece with flame-shaped
diamond burs of different gritsizes (DIATECH
multilayer diamond burs) under copious saline
irrigation until a smooth surface was obtained
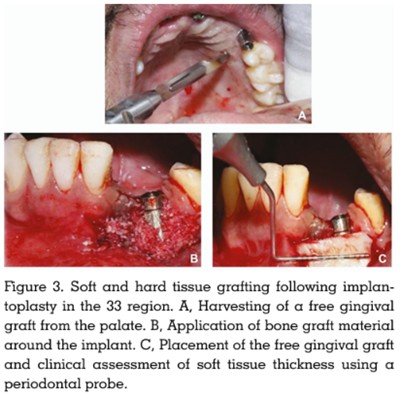
(Fig. 2B).5,8 A 13×8mm FGG was harvested (Fig.
3A) from the hard palate, and the donor site was protected with a treatment denture.10 Bone
graft (Osseograft- DMBM) mixed with injectable
platelet-rich fibrin (I-PRF) was placed in the area
of bone defect adjacent to the exposed implant
surface (Fig. 3B) and covered with the harvested
FGG (Fig.3C), which was then stabilized using
a 5-0 suture (Ethicon Absorbable surgical suture
USP). Eugenol-free, surgical dressing (COE
PAK Regular set)was placed. After 2 weeks,
the dressing was removed, and the site was
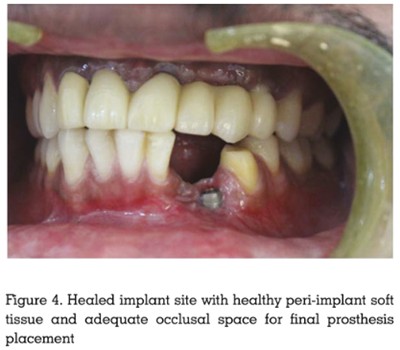
examined for healing. When reviewed after 1
month, a 90% closure of the exposed threads
was noted, without any uneventful complications
(Fig. 4).
In the prosthetic phase, a maxillary cement
retained fixed prosthesis and a mandibular
screwmentable cantilever fixed prosthesis
(Fig. 5A, 5B) were fabricated and cemented in
place. The coronal portion of the treated implant
surface, where complete soft tissue closure could
not be achieved, was left undisturbed (Fig. 5B)
to ensure access for hygiene and professional
maintenance. Endodontically treated #12 and
#34 were restored with porcelain-fused-to-metal
crowns. At the follow-up visit, a favourable soft
tissue response, reduced peri-implant probing
depth and bleeding, adequate width of attached
gingiva with sufficient vestibular depth,
preventing further muscular traction, were noted.

Despite the significant progress in periodontal
and peri-implant surgical regeneration
techniques, management of implant thread
exposure presents a significant clinical
challenge. In the present case, the primary
cause of bone loss and thread exposure was
likely the improper implant positioning coupled
with inadequate attached gingiva and excessive
muscle traction due to lip movements.4,11-13
Previous studies by Lin et al. have identified the
importance of adequate width of keratinized
mucosa in maintaining peri-implant health.11
Considering the unfavourable bone defect
morphology for regeneration, implantoplasty
was chosen due to its proven efficacy in
reducing bacterial recolonization and promoting
the integration of peri-implant tissues after
healing.1,7,9,14 Bianchini et al. reported that
implantoplasty significantly reduced marginal
bone loss and improved implant survival rates.15
Though effective, implantoplasty presents
several challenges, like potential weakening
of implant structure (particularly in narrow
diameter implants) and titanium particle release that could trigger an inflammatory response.16,17
Use of rotary diamond burs in descending grit
sizes effectively reduces surface roughness as
reported by Ramel Christian et al., while the final
polishing step helps minimize implant surface
roughness, thereby inhibiting biofilm formation
and maturation.15 Abundant saline irrigation
ensured minimized titanium particle deposition
and prevention of heat-induced damage to peri
implant tissues.8,17
Placement of xenograft - I-PRF covered with
an autogenous FGG enhances regenerative
outcomes. Studies by Kobayashi et al. showed
that
I-PRF releases growth factors that
stimulate cellular proliferation and migration,
potentially enhancing graft integration and soft
tissue healing.18 Autogenous tissue grafts are
considered as a gold standard for increasing
keratinized tissue width with a more predictable
outcome, thereby addressing the underlying
anatomical
deficiencies.6,8
Additionally,
augmentation of keratinized tissue around
implants significantly reduces bleeding on
probing, improves plaque control, and decreases
the incidence of recession.6,8,19
The limitation of this case report is the short
follow-up period, preventing long-term outcome
assessment. However, this case emphasizes
the necessity of thorough pre-surgical planning
to prevent thread exposure. A comprehensive
evaluation of soft tissue biotype, vestibular
depth, and muscle attachments prior to implant
placement to identify and manage risk factors
through preventive strategies like vestibuloplasty
and soft tissue grafting during the initial time of
implant placement could effectively lessen the
subsequent complications.4,7,8
This clinical case highlights the effectiveness
of combining implantoplasty with free gingival grafting in the management of implant thread
exposure, thus suggesting its potential to serve as
a minimally invasive alternative to more complex
reconstructive procedures. However, further
studies with large sample sizes and extended
follow-up periods are needed to establish an
evidence-based therapeutic protocol for implant
thread exposure and soft tissue management.
DECLARATION OF GENERATIVE AI AND AI
ASSISTED TECHNOLOGIES IN THE WRITING
PROCESS
During the preparation of this work, the author(s)
used ChatGPT and Claude to summarize a few
portions of the original written draft of the case
report. All content generated with the assistance
of these tools was reviewed and edited by the
authors to ensure accuracy with the scholarly
standard of the work. The authors take full
responsibility for the content of the manuscript.