Accurate transfer of maxillomandibular relationships is critical for predictable outcomes in prosthodontics. The conventional facebow is technique-sensitive and approximates the true hinge axis, introducing potential inaccuracies.¹ This case report describes a fully digital workflow using Cone Beam Computed Tomography (CBCT) as a precise alternative for the full arch fixed rehabilitation of a 54-year-old male with severe dental wear and loss of occlusal vertical dimension, including the replacement of a molar with an implant prosthesis. The treatment involved a prosthetically driven implant plan and integrated intraoral scans with the patient’s CBCT data for a virtual articulation based on true anatomical landmarks, bypassing the physical facebow. A full arch monolithic zirconia prosthesis was designed based on a canine-guided occlusal scheme, with an implant-protected occlusion for the implant crown. The prostheses were milled and delivered concurrently, exhibiting excellent fit with minimal occlusal adjustment. This CBCT-based digital workflow represents an accurate, efficient, and viable alternative to conventional methods for complex prosthodontic rehabilitations.
Key words: Digital facebow transfer; Virtual articulator; Full-arch mandibular rehabilitation; Digital prosthodontics
Successful
prosthodontic rehabilitation
depends on the accurate transfer of the
patient’s maxillomandibular relationships to an
articulator. This is especially critical in full arch
reconstructions where re-establishing a stable
and functional occlusion is paramount.
For decades, the mechanical facebow has been
the standard for capturing the spatial relationship
of the maxillary arch to the craniofacial structure.
However, the conventional facebow has inherent
limitations; it is a technique-sensitive device
prone to operator-induced errors.¹ Furthermore,
it relies on anatomical averages rather than the
patient’s true condylar position. These limitations
can introduce inaccuracies that are magnified
through subsequent laboratory steps, resulting
in a final prosthesis with occlusal discrepancies.
Such errors necessitate extensive intraoral
adjustments, which can compromise the integrity
of modern restorative materials. Minor variations
in hinge axis transfer can have a substantial
impact on occlusal outcomes, particularly in full
mouth rehabilitation cases.2,3
The integration of Cone Beam Computed Tomography (CBCT) with Computer-Aided
Design/Computer-Aided Manufacturing (CAD/
CAM) software offers a higher level of precision.
This report presents a clinical case demonstrating
a CBCT-guided virtual articulation protocol for a
complete mandibular rehabilitation, showcasing
it as an accurate alternative to the conventional
facebow.
A 54-year-old male patient presented with a chief
complaint of a missing lower right second molar,
significant wear on his remaining lower teeth,
and decreased chewing efficiency. His medical
history was non-contributory.
Clinical and radiographic examination revealed
a missing mandibular right second molar (tooth
47), moderate to severe generalized attrition
of the remaining mandibular teeth, and a loss
of occlusal vertical dimension (OVD). The final
diagnosis was a partially edentulous mandibular arch complicated by severe dental attrition, with
the edentulous space for tooth 47 planned for a
single-tooth implant.
The treatment plan consisted of a full mandibular
arch fixed prosthesis rehabilitation using
monolithic zirconia crowns to restore function,
aesthetics, and the correct occlusal vertical
dimension (OVD). The plan utilized a fully
digital workflow, incorporating a prosthetically
driven approach for the implant placement.1,3
A canine-guided occlusion was planned for the
full arch rehabilitation, with a specific implant
protected occlusion for the implant prosthesis.4,5
The workflow replaced the conventional facebow
transfer with a CBCT-based virtual mounting
protocol to ensure maximum accuracy.
The treatment followed a systematic digital
protocol, integrating clinical procedures with
laboratory software.
Diagnostic digital impressions were taken using
an intraoral scanner. A Lucia jig was used for
neuromuscular deprogramming to facilitate the
recording of a verifiable centric relation (CR)
position.

A new, increased OVD was determined based
on phonetic and aesthetic parameters. A hard
acrylic occlusal splint was fabricated at the
proposed OVD, which the patient wore for four
weeks to confirm comfort and adaptation.
CBCT scan of the patient’s craniofacial structures
was acquired. In the laboratory, the patient’s
CBCT data (DICOM format) was imported into
EXOCAD v3.3 software and aligned with the
intraoral scan data (STL format). This data
fusion creates a comprehensive digital model
of the patient’s anatomy. The software allows
for the direct identification of true anatomical
landmarks from the CBCT scan, such as the
center of the condylar heads and an anterior
reference point. By using these patient-specific
points, the digital maxillary cast is positioned on the virtual articulator in a precise spatial
relationship to the patient’s true hinge axis.6
This transforms the articulator into a high
fidelity digital representation of the patient’s
stomatognathic system.

After the new OVD was verified, the digital design
of the final crowns was completed. This digital blueprint served as the basis for a prosthetically
driven implant plan.¹ The implant for tooth
47 was virtually positioned to ensure it would
support the ideal prosthetic form and function.
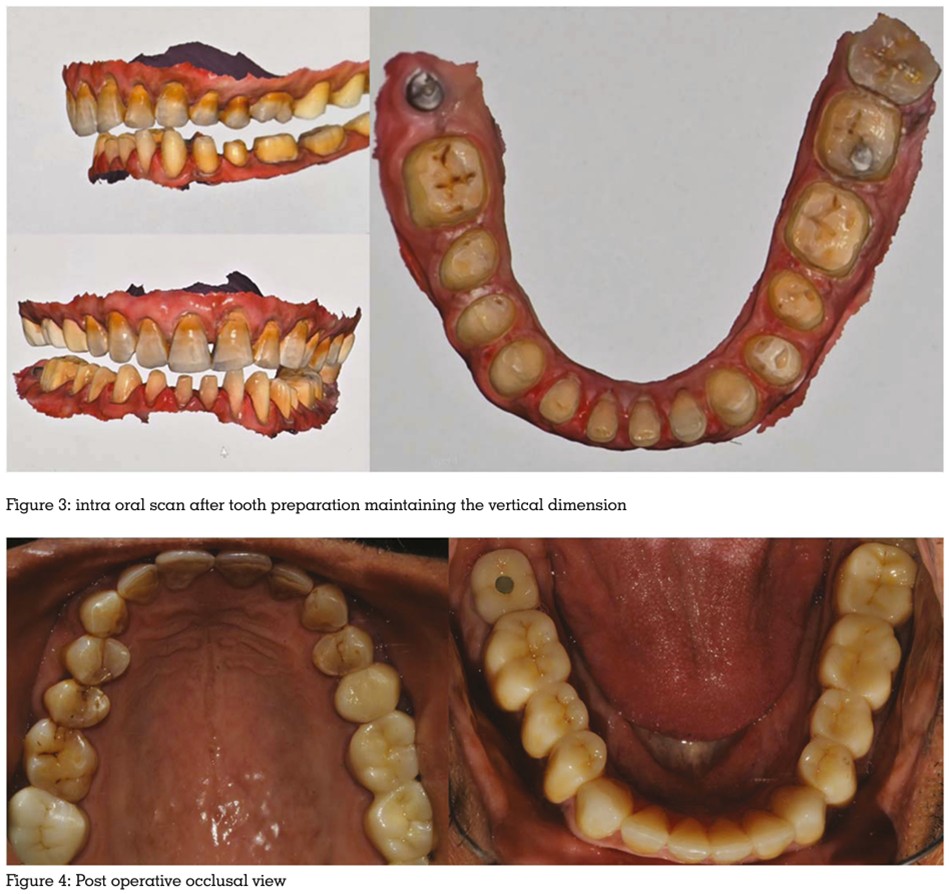
The implant was placed following the
prosthetically driven planning. The fixed
restoration using crowns was carried out simultaneously while the osseointegration period
was being completed. The full mandibular arch
was prepared for monolithic zirconia crowns in a
single appointment. First the anterior section was
prepared and new anterior jig was fabricated
on the prepared teeth to maintain the new
established OVD and centric relation followed by
preparation of posterior teeth. Definitive digital
impressions of the prepared arch, the opposing
arch, and a bite registration at the verified OVD
were then captured using the new anterior jig
and bite registrations, followed by temporization
with CAD/CAM-milled PMMA crowns.
With the casts virtually articulated, the final
design for the full arch monolithic zirconia
prosthesis was completed, adhering to the
principles of a canine-guided occlusion.4
Gnathological Concept was followed and
executed within a Reorganized Approach to full
mouth rehabilitation. The single implant crown
was designed following the principles of implant
protected occlusion to manage biomechanical
stresses.5 A pre-sintered “bisque” try-in was
conducted to verify fit and function. Following
minor adjustments, the prosthesis was returned
for final staining and glazing. The implant
prosthesis was delivered along with the final
cementation of the crowns.

The full mandibular rehabilitation was completed
successfully, with the patient reporting high
satisfaction with the comfort and function of
the new prosthesis. The predictable outcome
is attributed to the precision of the fully digital
workflow.
The choice of a canine-guided occlusal scheme
for the natural dentition was deliberate, aiming
to provide disocclusion of the posterior teeth
during excursive movements, thereby reducing harmful lateral forces on the new restorations.4
For the implant prosthesis, an implant-protected
occlusion was meticulously developed. This
involved managing occlusal contacts to ensure
forces were directed along the implant’s long
axis and to account for the lack of a periodontal
ligament, which is critical for mitigating
biomechanical stress and ensuring the long
term health of the surrounding bone.5 The
prosthetically driven planning was instrumental,
as it ensured the implant was placed in the ideal
position to support the final restoration, rather
than compromising the prosthetic design based
on available bone alone.1,3
The primary advantage of this technique is the
enhancement in accuracy. By using the patient’s
own condylar anatomy from the CBCT scan
as the definitive reference, the approximation
errors inherent in mechanical facebows
are eliminated.6,7 This heightened precision
translates into a more accurate final prosthesis,
requiring minimal chairside adjustment. This
not only saves clinical time but also preserves
the glazed surface integrity of the monolithic
zirconia. This outcome aligns with studies
demonstrating the high accuracy of CBCT
based virtual mounting techniques compared to
conventional methods.7
This case applies the principles described in
the literature for mounting maxillary scans on
a virtual articulator, creating a more complete
“virtual patient.”2,6 The digital process also
enhances efficiency and repeatability by
removing several physical steps and the potential
for error. The digital record is permanent and
can be recalled perfectly, ensuring the transfer
process is highly repeatable. This technique
makes high-precision prosthodontic care more
accessible, as CBCT technology is increasingly
available in diverse practice environments.
The integration of CBCT imaging with CAD/
CAM software for virtual articulation provides a
clinically viable and accurate alternative to the
conventional facebow transfer. As demonstrated
in this full arch mandibular rehabilitation,
which included the successful integration of a
prosthetically driven single-tooth implant, the
all-digital approach facilitates the fabrication of
a highly precise prosthesis, minimizing clinical
adjustments and improving workflow efficiency.
This case integrates the foundational principles
of gnathology with modern digital concepts.
This technique has the potential to become
a new standard of care, contributing to more
predictable, faster and successful outcomes in
extensive restorative treatment.