Rehabilitation of anterior ridge defects poses significant challenges due to associated loss of hard and soft tissues, impacting esthetics, phonetics, function, and hygiene. Conventional fixed or removable prostheses often fail to address these multifactorial demands. The fixed-removable prosthesis, exemplified by the Andrews Bridge system, offers a practical alternative by combining the stability of a fixed framework with the adaptability of a removable segment. This clinical report describes the management of a patient with a Siebert Class III anterior maxillary ridge defect using the Andrews Bridge philosophy. The prosthesis included fixed retainers connected by a bar and a removable acrylic segment retained via a sleeve attachment. This design allowed for optimal esthetics, phonetics, improved oral hygiene, and favorable force distribution. The Andrews Bridge system proved to be an effective, conservative, and versatile solution for complex anterior defects where conventional prostheses may be inadequate.
Key words: andrews bridge, fixed removable prosthesis, bar and sleeve attachment, esthetics.
Tooth loss due to caries, periodontitis,
trauma, or surgery often leads to alveolar
ridge resorption, compromising esthetics,
speech, and function. Traditional treatment
includes surgical augmentation or prosthetic
rehabilitation.1 However, surgical options may
be unpredictable or costly in severe resorption
cases. Prosthodontic alternatives like fixed
partial dentures, implant-supported prostheses,
and fixed-removable systems are considered
based on individual needs. The fixed-removable
system, such as the Andrews Bridge introduced
by Dr. James Andrews, combines fixed retainers
with a removable pontic segment, offering both
esthetic results and ease of hygiene maintenance
in ridge defect cases.2
A 49-year-old female patient presented to the
Department of Prosthodontics with the chief
complaint of missing lower front teeth and dissatisfaction with her smile. She had previously
worn a removable partial denture replacing teeth
from right lateral incisor to left lateral incisor
which was discontinued due to discomfort and
poor retention. The patient strongly preferred a
fixed solution but declined surgical and implant
therapy due to financial constraints.
Intraoral examination revealed a partially
edentulous mandibular anterior region (right
lateral incisor to left lateral incisor) with moderate
ridge resorption. An existing fixed prosthesis
was noted in the maxillary anterior region
(right lateral incisor to left lateral incisor). An
orthopantomograph (OPG) confirmed a Siebert
Class III ridge defect in the lower anterior arch.
Right and left mandibular canines evaluated as
suitable abutments.
Considering the patient’s esthetic demand,
hygiene concerns, and reluctance for surgical
interventions, a fixed-removable prosthesis
following the Andrews Bridge design was
selected. This included porcelain-fused-to-metal
(PFM) retainers on right canine and left canine
connected by a bar, and a removable acrylic
pontic segment replacing the four missing
anterior teeth.
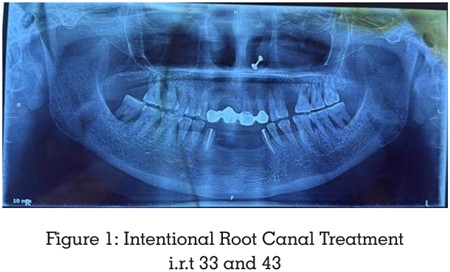
Intentional root canal treatment was performed
on teeth right canine and left canine [Figure
1]. Tooth preparation was done to receive PFM
crowns. A diagnostic impression was made
to facilitate bar alignment and wax-up. Final
impressions were recorded using the double-mix
single-step technique with polyvinyl siloxane
(3M ESPE Express, India).
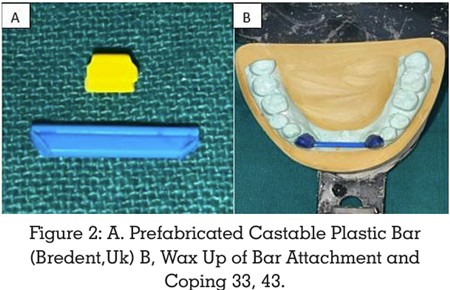
Master casts were poured using Type IV dental
stone (Neelkanth,India)and articulated. Wax
patterns for the retainers were fabricated, and a
prefabricated castable plastic bar (Bredent, UK)
was incorporated parallel to the ridge [Figure
2]. A space of 2–3 mm was maintained between
the bar and residual ridge to ensure hygiene
access.3
The entire metal framework was cast using
cobalt-chromium alloy (Wirobond C, Sweden),
and a metal try-in was conducted. Shade
selection was done using the VITA shade guide.
A wax-up of the missing anterior teeth was
prepared and evaluated intraorally for esthetics
and phonetics. The ceramic build-up of the PFM
bridge was completed, and the fixed component
was cemented with glass ionomer luting cement
(3M Ketac, India) [Figure 3].

The removable acrylic segment was processed
using heat-cure resin (DPI, India). The undercut
beneath the bar was blocked out, and a clip was
picked up into the denture using self-cure acrylic
resin. The final prosthesis was polished and
delivered after evaluating esthetics, phonetics,
retention, and comfort [Figure 4].
The patient was instructed on insertion and
removal of the prosthesis and advised to use
an interdental brush for cleaning beneath the
bar.4 Oral hygiene instructions were reinforced,
and the importance of regular follow-up was
emphasized to monitor tissue health and
prosthesis integrity.1

Ridge defects following tooth loss can be classified
according to Siebert’s classification.5 A Class III
defect, characterized by combined horizontal
and vertical bone loss, presents significant
challenges for prosthetic rehabilitation. These
defects compromise esthetics, phonetics, and
function, especially in the anterior region.6
Traditional fixed prostheses may appear
elongated or esthetically unpleasing in
such cases. Removable prostheses, while
compensating for tissue loss, may lack retention
or patient acceptance. The Andrews Bridge
system bridges this gap by combining a fixed
splint with a removable pontic segment, making
it suitable for localized defects.7
This approach is particularly advantageous in
cases where:8
The removable segment allows for easy
maintenance and future relining if soft tissue
changes occur. It improves esthetics by enabling
customization of pontic contour and flange
extension, which enhances lip support and
speech. Additionally, occlusal forces are directed
favorably along the long axis of the abutments,
improving biomechanical stability.7
Common failures of the system are mechanical
in nature, often due to inadequate soldering
or improper clip fit. These can be mitigated by
using single casting techniques and quality
attachment systems.
In this case, the patient benefited from all the
advantages of the system—enhanced esthetics,
phonetics, functional efficiency, and ease of
maintenance. The prosthesis restored her smile,
improved confidence, and met her expectations
without the need for surgical interventions.8
The Andrews bridge system is an efficient fixed
removable prosthetic solution for managing
localized anterior ridge defects, especially in
patients unwilling or unsuitable for implant or surgical options. It successfully restores
esthetics, speech, and function while allowing
for excellent hygiene maintenance. With proper
case selection, careful fabrication, and patient
education, it offers long-term clinical success
and high patient satisfaction.