Background: Traditional suction or adhesive-retained
finger prostheses often fail in cases of very short or
irregularly shaped residual stumps, compromising
retention, function, and patient satisfaction.
Aim: To present an innovative technique for retaining
finger prostheses using custom-cast rings with
integrated mesh, specifically designed to address
retention challenges in patients with anatomically
compromised finger stumps.
Methodology: This case series reports on the prosthetic
rehabilitation of patients with missing fingers and
short/irregular stumps using castable ring-retained
prostheses. Castable rings with integrated mesh were
fabricated to fit securely over the stump, incorporating
inner and outer finish lines for optimal silicone
merging. A flexible wax pattern was utilized to sculpt
the prosthesis, followed by silicone processing. In
cases with extremely short stumps, buddy rings were
connected to adjacent fingers without impeding
natural movement, enhancing retention. The castable
ring design facilitated superior prosthesis retention,
ease of insertion/removal, and prevented fraying
of the silicone edges, thereby extending prosthesis
longevity. The buddy ring adaptation enabled prosthetic use in minimal-stump scenarios while
maintaining tissue compatibility and joint mobility.
Conclusion: Castable ring-retained prostheses offer
a practical, durable, and patient-friendly alternative
for restoring form and function in cases where
conventional retention methods are unsuitable.
This approach significantly improves prosthesis
stability, aesthetics, and wearer comfort, especially
in challenging anatomical conditions.
Key words: finger prosthesis, castable ring, short stump, mesh retention, silicone prosthesis, buddy ring, prosthetic rehabilitation, irregular finger amputation
Congenital or trauma induced defects are
commonly seen in the form or missing fingers/
toes. Rehabilitation of such defects by a prosthesis
is not common in India due to unawareness
amongst the general population, accessibility to
treatment and cost of the treatment.
Surgical reconstruction of amputated digits is
often not recommended for many patients due
to potential postoperative complications and the unpredictability of esthetic outcomes.1,2 In these
patients a passive prosthesis is advocated.1
Passive finger prosthesis can be fabricated
in acrylic or silicone material. Though acrylic
has more durability as compared to silicone
prosthesis made of silicone material has more
lifelike appearance, function and feel.
Retention for silicone finger prosthesis can be
achieved by positive fit of retention sleeves, using
implants and adhesives.3 Artificial jewellery like
finger rings, wrist bands or bangles can be used
to gain additional retention for the finger or hand
prosthesis. They are also used to mask the seam/
junction between the prosthesis and the finger or
hand. The most common problem encountered
with finger rings is the difficulty to get the exact
size which will fit the stump and the prosthesis.
This happens because the stump is irregularly
shaped most of the times with the terminal part
of stump being broader than the base of finger.
Hence a broader ring is required which will pass
over the enlarged part of the stump but such a
ring has a loose fit at the bottom part of the stump.
This leads to the movement of prosthesis over the
stump. Castable rings are a plausible solution
for this wherein the ring can be customized to
have a fit as close as possible to the irregularly
shaped stump. In situations where no stump is
present retention is achieved by either implants
or adhesives or by using adjacent finger. Use of
customized rings in such situations is extremely
useful as not only do they provide retention, but
can be designed in such a way as to provide
support to silicone material too.
A patient presented with index finger of the left
hand amputated at proximal phalange of the
left hand. The patient had lost her finger due to
trauma. Though the patient was able to function
with the partially amputated finger it was not
esthetically pleasing. It was decided that a
silicone finger prosthesis should be fabricated for the patient retained with a castable ring.
Impression and Model:
Two impressions of the fingers of the left hand
along with the stump of the index finger were
made using irreversible hydrocolloid (Tropicalgin – Zhermack) impression material. The patient
was advised to keep fingers relaxed while the
material set. Once the material set, the patient
was asked to wriggle fingers a little and pull
the hand out. A similar impression of the right
hand was also made to help during modeling
of the pattern of finger. The impressions were
evaluated for any porosities or tears and dental stone (Kalstone – Kalabhai) was poured into
the impressions of left and right hand to make
models. The second left hand impression was
poured in industrially available tin silicone (Tin
Cure RTV Liquid Silicone Rubber – Asia Silicone
Chemicals Co.) to make a flexible mold.

Making of custom made casted ring:
Outline was marked to decide the position of the
ring. Trimming of the model in the outlined portion
by 1mm was done with a tungsten carbide bur to
ensure an active fit of the ring, hence rendering
it more retentive. A single layer of baseplate wax
was added on the stump, from above the upper
border of the ring, to make space for the silicone
material and achieve an internal finish line in
the casting (Fig. 1a).
The stump with the wax was duplicated to make a
refractory cast. Wax pattern was then fabricated
on the refractory cast. Around 2 to 3 mm of width
was kept for the ring and an extension of around
3 to 4 mm was given in the area where there
was baseplate wax, for retention of the silicone
material. Holes were made in the extension large
enough for silicone to flow through. The pattern
was then casted in chrome cobalt alloy, and
finished (Fig. 1b). It was tried on the patient’s
finger to check for fit and comfort (Fig. 2a).
Making of Wax Pattern of the Finger:
The flexible model of stump was used to fabricate
the silicone part of prosthesis as the ring would
not fit on a rigid model since it was made on a
smaller model. The casted ring was placed on
the model and evaluated for the fit whether it
was exactly same as that on patient’s finger.
Base plate wax was used to make the pattern
of the finger. The model of the other hand was
used for guidance while carving the pattern to
replicate the size, form and patterns of the finger.
It was ensured that the wax flowed through the holes made in the ring. After trying the pattern
on the patient’s finger, it was relined from inside
using fluid wax to record all the fine details of
the stump (Fig. 2b). This helped to improve the
adaptation of the prosthesis to the finger stump.
The pattern was then processed.

Processing:
Dental stone was flowed in the pattern on the
tissue side and allowed to set. The pattern
along with the stone was then flasked in the
conventional manner and dewaxed. The silicone
material (Technovent Silicone Rubber) was then packed in the obtained mould. Intrinsic stains
were used before packing to achieve a basic
shade of the finger. The silicone was allowed to
cure for 24 hours at room temperature.
Fabrication of artificial nail
After the wax pattern was completed and before it
was processed the artificial nail was fabricated.
The nail bed was carved in the wax pattern and
a mould of the wax pattern was made in putty
elastomer. A cast of the same was made on
which a wax pattern of the nail was fabricated
and finished. The wax pattern along with the
cast was flasked and nail was fabricated using
compression molded technique. Shade matching
was done while mixing the heat cure resin at the
time of packing. To replicate the colour of the
nail tooth coloured, clear and pink acrylic was
mixed in varying proportions. After processing
the nail, it was finished and polished.
Finishing and Delivery:
On retrieval of the prosthesis, excess was
trimmed with scissors and silicone trimming
burs. The prosthesis was then tried on the
patient. This was followed by extrinsic staining
to improve the match of the shade with adjacent
fingers. The extrinsic stains were sealed with a
sealer. After the sealer hardened, the artificial nail was attached in the prepared nailbed using
polyacrylate cement. The prosthesis was then
delivered to the patient (Fig 3). The patient was
given instructions about post insertion care of
prosthesis.

A patient presented with almost completely amputed little finger of left hand. The patient had lost her finger to trauma which had also resulted in formation of scar tissue covering lateral side of hand. Due to the size and shape of the stump it was not possible to make a conventional silicone prosthesis taking support from stump or a castable ring supported prosthesis placed on the stump. It was therefore decided to take support from the adjacent ring finger by making a castable ring with extension for little finger prosthesis. Impressions were made as previously described.
Making of casted ring
After trimming of cast (to compensate for
compressibility of tissues) resin pattern was
adapted in the shape of a ring. This was then tried on the patient (Fig. 4a). The accurate fit
of the resin ring confirmed that the cast was
trimming was adequate.
This trimmed cast was then duplicated to make
the refractory cast. On the refractory cast, wax
pattern was made in the form of ring on ring
finger. A slightly smaller ring (double/buddy ring)
was fabricated on stump which was connected
to the ring on adjacent finger. Metal extensions
in the form of mesh were made on superior and
inferior border of ring made on stump. Casting
was done with cobalt chromium alloy (Fig. 4b).
The finished and polished rings were tried on
patient.
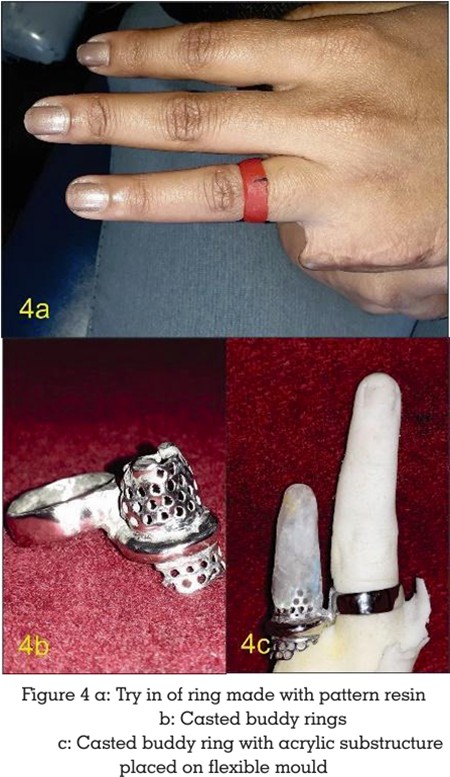
Fabrication of acrylic substructure
To reduce the weight of prosthesis, it was decided
to make the prosthesis hollow by making an
acrylic substructure. To determine the size of
acrylic substructure, wax up of the little finger
was done. After making putty index of the finger,
the wax pattern was removed and pattern for
substructure was made which engaged the
superior mesh of the ring on the stump. This
pattern was checked with putty index on finger
to evaluate its position and size. It was then
processed with clear heat cure acrylic resin. This
substructure was kept hollow to reduce its weight
(Fig. 4c).
Fabrication of wax pattern
The ring with acrylic substructure was placed on
flexible model and wax pattern was fabricated.
The pattern was processed and silicone
prosthesis was fabricated as stated above (Fig.
5a).

The artificial nail was attached and prosthesis
was given to the patient (Fig. 5b).
The challenges faced while fabricating finger prosthesis mainly pertains to retention of the
prosthesis. The property of retention is as
important as esthetics for finger prosthesis.
Various techniques are used to ensure retention
of prosthesis. In silicone prosthesis, vacuum
is commonly used to retain prosthesis. Since
silicone is an elastic material it can be stretched
over the stump to create negative pressure.
To ensure that the demarcation between the
prosthesis and thumb is obliterated, the margin
of the prosthesis is thinned. The repeated wear
and removal cause this thin margin of prosthesis
to fray and tear. Prolonged use of such silicone
prosthesis which retain by suspension method
may lead to atrophy of tissues4. In situations
where short stump is tapering, suspension
method cannot be effectively used.5 Alternate
methods of retention are adhesives for silicone
prostheses. Adhesives are preferred over plain
surfaces rather than curved surfaces like that
of finger stump. Also placing prosthesis with
adhesive is difficult as the thin margins may
fold or distort while placement. It is important
that the adhesive is thoroughly cleaned from
the stump and prosthesis to maintain health of
tissues. So adhesives are not preferred means of
retention for finger prosthesis. Newer methods
include suspension socket which create suction
between stump and socket.4,6 The inner diameter
of socket is smaller than the stump which helps
in creating the suction.7 The socket is lined
form outside with silicone material to attain the
required the contour. Such type of suspension
prostheses may cause soft tissue atrophy of the
residuum after prolonged use.7 Other method of
achieving retention is the use of finger rings. The
primary advantage of employing finger rings is
that they help to obscure the junction between
the prosthesis and the stump while maintaining
tissue health, as retention is not solely dependent
on suction. In cases where the prosthesis is
slightly loose the ring helps in securing the
prosthesis to the stump. Finger rings available
locally can be used for the same. Challenge lies in finding a finger ring which will fit the stump
since the stump is unlike the normal finger. The
stumps are usually irregularly shaped especially
due to irregular scar tissue formed post trauma.
Considering the above factors, in these patients
we decided to use a ring to enhance the retention
of the prosthesis while maintaining the health of
the residuum. After the impressions were made
and models were obtained the patients were
asked to get a ring which would fit the stump.
But the rings available in the market did not
precisely fit the stump and were either loose
or too tight to pass through the stump. Hence
it was decided that a ring has to be casted
which will fit the stump precisely. After the ring
with extension was casted it was tried out on
the patient. The extension was in the form of
mesh all along the circumference of ring. Such
extensions provide better support to silicone as
compared to extensions made with wires and
loops.6 Proper fit was obtained by compressing
the tissues sufficiently to get good retention. The
casted ring had inner and outer finish line on the
extension with holes in the extension. The finish
lines ensured that silicone ends on a butt joint
with ring giving a life like appearance. This also
ensured uniform thickness of silicone at border
which will prevent fraying of material at the
border. The holes were made in the extension
for mechanical interlocking of silicone with
ring. To precisely duplicate the fit of the ring
on finger stump a flexible model of the stump
was made using industrial grade silicone. This
not only allowed the ring to seat in the correct
position but also gave the most true form and
contour of the stump for fabricating the silicone
prosthesis. (Though it is not possible to exactly
duplicate the compressibility of stump). There
are problems encountered with double/buddy
rings like compromised stability of prosthesis
with repeated flexion and extension of hand and
fingers.5 In this case the stump was too short to
cause any hindrance to the stability of prosthesis.
Artificial nail for the finger was fabricated using heat cure resin as mentioned before. Even
though prefabricated nails are available it
becomes difficult to match the colour with the
remaining nails. The shape and contour of nail
can be manipulated as desired which becomes
difficult with prefabricated nails. The prosthesis
requires six monthly recall check up to maintain
the health of residuum and the prosthesis can
be changed after 3-4 years depending upon the
colour and flexibility of silicone.
Employing a castable ring for retention in
finger prostheses provides multiple clinical and
functional advantages. The primary advantage
is the predictability of retention after the insertion
of prosthesis. As the prosthesis does not depend
on flexibility of silicone for retention, the amount
of retention remains constant throughout its
life. The common problem of frayed border of
silicone prosthesis with use is eliminated as
the silicone ends on ring rather than directly on
tissue and the ring is easier to handle rather than
silicone directly while placement and removal of
prosthesis. The casted finger ring also maintains
the health of residuum which is compromised in
other methods of retention like the suspension
socket. Considering all these points ring should be preferred means of retention for finger
prosthesis when the stump is small or support
from adjacent finger is required.
Conflict of Interest
The authors declare no conflict of interest.
Written informed consent was obtained from
the patients for publication of case details and
clinical photographs.