PURPOSE: To evaluate the impact of varying
concentrations of UHMWPE (ultra-high-molecular
weight polyethylene) filler particles on provisional
self-cure PMMA’s mechanical properties by analyzing
the flexural strength and hardness of the specimens
along with the scanning electron microscopic analysis.
MATERIALS AND METHODS: Four groups of
specimens (n=16 per group) were prepared using
PMMA incorporated with different concentrations of
UHMWPE - Control group (Pure PMMA), 10% UHMWPE
group, 20% UHMWPE group, 30% UHMWPE group.
Flexural strength was measured using a Universal
Testing Machine under a three-point bending setup
while hardness was evaluated using the Shore A
hardness testing machine and the surface of fractured
samples was analyzed using a scanning electron
microscope (SEM). One-way statistical ANOVA test
was done to find the difference between groups,
followed by Tukey’s post hoc test for multiple pairwise
comparison.
RESULTS: The highest flexural strength was reported
in 10% UHMWPE group followed by the Control PMMA
group, 20% UHMWPE group and 30% UHMWPE group.
Higher concentrations of UHMWPE (20% and 30%)
showed a decline in flexural strength, with values
similar to or lower than the control group. In contrast,
Shore A hardness values increased progressively
with UHMWPE concentration, with 30% UHMWPE
group achieving the highest values (92.8 ± 0.73). SEM
evaluation showed uniformly dispersed UHMWPE filler
particles in PMMA matrix at 10% UHMWPE group.
CONCLUSION: 1) The incorporation of 10% UHMWPE
significantly enhances flexural strength. 2) Increase
in UHMWPE content to 20% and 30% led to a decline
in flexural strength. 3) A consistent increase in Shore
A hardness was observed with increasing UHMWPE
concentration. The highest hardness values were
recorded at 30% UHMWPE.
Key words: PMMA, ultra-high-molecular weight polyethylene, flexural strength, shore a hardness, provisional restorations, reinforcement, SEM analysis.
Provisional restorations are a critical component
of prosthodontic and restorative dentistry, serving
as interim prostheses that protect prepared teeth,
restore function, maintain esthetics for the period
until the fabrication of the definitive prostheses.
Among the various materials available,
polymethyl methacrylate (PMMA) is widely used
due to its ease of fabrication, cost-effectiveness,
and acceptable esthetic properties.1,2 To
enhance PMMA’s mechanical properties,
various reinforcement strategies have been
explored, including the incorporation of fibers
(glass, polyethylene, carbon), nanoparticles
and polymer blends. These modifications
have demonstrated improvements in strength,
wear resistance, and overall durability.2 One
promising reinforcement material is ultra-high
molecular weight polyethylene (UHMWPE), a
polymer recognized for its superior mechanical
properties, including high flexural and tensile
strength, impact resistance, and biocompatibility.
UHMWPE is extensively used in biomedical and
dental applications due to its excellent wear
resistance and structural integrity.3 Structurally,
UHMWPE has an extremely long polymer chain and high molecular weight, contributing
to enhanced toughness and crack resistance.
When incorporated into PMMA, UHMWPE acts
as a reinforcing phase by interlocking polymer
chains which contributes to increased load
bearing capacity and mechanical durability.
[4] This study aims to evaluate and compare
the flexural strength and hardness of PMMA
reinforced with different concentrations of
UHMWPE (10%, 20%, and 30%). This study
fills the gap in research by analyzing whether
UHMWPE can be used in provisional PMMA to
increase its flexural strength and hardness and
capable of withstanding functional loads while
maintaining surface integrity and esthetics.5,6
This comparative in vitro study was conducted
in the department of prosthodontics and crown
and bridge in collaboration with a mechanical
strength testing lab. The sample size for this
study was determined based on the mean
and standard deviation values reported in
a previous study by Apimanchindakul C. et
al.7 A priori power analysis was performed
using G*Power 3.1.9.7 software, considering a significance level (α) of 0.05, a power (1−β)
of 0.90, and an estimated effect size (f) of 0.40
derived from previously published literature.
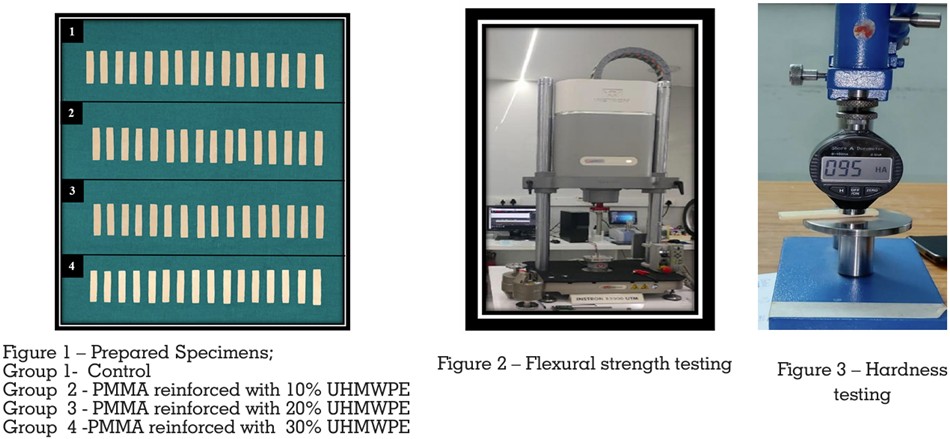
The study included four groups each consisting
of sixteen samples prepared according to ISO
20795-1:2013 guidelines for mechanical testing
of resin-based dental materials. [Figure 1] The
groups were categorized as follows:
Group 1 (Control): Pure PMMA without any
reinforcement.
Group 2: PMMA reinforced with 10% UHMWPE
by weight.
Group 3: PMMA reinforced with 20% UHMWPE
by weight.
Group 4: PMMA reinforced with 30% UHMWPE
by weight.
For the preparation of reinforced PMMA, the
required amounts of PMMA powder (DPI® Self
Cure Acrylic Resin Polymer, Dental Products of
India Ltd) and UHMWPE powder (Dyneema®
UHMWPE powder, DSM Dyneema,Geleen,
Netherlands) for each group were accurately
weighed using a high-precision digital balance
with an accuracy of 0.01 g. The powders were
mixed using a turbo mixer (Biobase Vortex
Laboratory Mixer Model: MX-S) at 300 rpm for
5 minutes to break down any agglomerates and
ensure uniform dispersion. After dry mixing,
the appropriate amount of methyl methacrylate
(MMA) monomer (DPI® Self-Cure Acrylic Resin
Monomer) was added in a monomer-to-powder
ratio of 1:3. The mixture was stirred gently to
avoid air entrapment and ensure even wetting
of the powders. The mold was lubricated with
petroleum jelly to facilitate easy removal of
the specimens. The prepared mixture was then
poured into stainless steel molds (64 mm × 10
mm × 3.3 mm) and subjected to a pressure of
2 MPa using a hydraulic press (Carlo De Giorgi
S.R.L., Italy) with a cellophane sheet as a separating medium to prevent the sticking of the
resin to the press and for uniform distribution.
The self-cure polymerization process occurred
at room temperature (23°C) over 30 minutes
without the need for external heating. Once
polymerized, the specimens were removed from
the molds, trimmed, and polished (JT-24B Dental
High-Speed Cutting and Polishing Machine,
NSKI) on wet ground polishing machine. Silicon
carbide paper discs of 600, 800, 1000, and 1200
grits sizes were used. Diamond polishing paste
(Polyshine® Acrylic Polish, MDC Dental) was
used on the same machine for final polishing
to achieve smooth, uniform surfaces. Scanning
electron microscopy (Carl Zeiss Ltd., 40 VP, Smart
SEM) was used to investigate the distribution of
the UHMWPE particles in the cured PMMA resin
samples.8-10
Flexural strength was evaluated using a three
point bending test performed on a Universal
Testing Machine (Instron, USA). The specimens
were positioned on a support span of 50 mm, and
a force was applied at the center with a crosshead
speed of 1 mm/min until fracture occurred. Each
sample was tested individually, and the average
flexural strength of each group was recorded.
[Figure 2]11,12 Hardness was measured using a
Shore A durometer (Teclock, Japan; Model: GS
709). Each specimen was placed on a flat, non
resilient surface, and the durometer was applied
perpendicularly with a steady pressure. The
contact time was maintained for 15 seconds, after
which the hardness value was recorded. Three
readings were taken at five different locations on
each specimen to account for potential surface
variations, and the average hardness value was
calculated for each group.13 [Figure 3]

The recorded flexural strength and hardness
values were subjected to statistical analysis
using the software SPSS 26.0 (SPSS Inc.,
Chicago, IL, USA). One-way statistical analysis of variance (ANOVA) test was done to find the
difference between groups. Descriptive statistics
for flexural strength (mean, standard deviation,
and 95% confidence interval) across the four
groups are presented in Table 1. The test
revealed a statistically significant difference
among the groups (P < 0.05). [Figure 6] Post hoc
analysis using Tukey’s test [Table 2] confirmed that
the 10% UHMWPE group exhibited
significantly higher flexural strength compared to other groups (P < 0.05). Cohen’s d effect size
analysis further supported these findings. These
results confirm that 10% UHMWPE reinforcement
significantly improves flexural strength, while
30% UHMWPE adversely affects it. For hardness,
a similar statistical approach revealed
significant differences among the groups (P <
0.05). Descriptive data are shown in Table 3. The
highest Shore A hardness value was observed
in the 30% UHMWPE group, followed by 20%,
10% and the control groups. [Figure 4] Tukey’s
post hoc analysis [Table 4] indicated significant
differences between all groups. Cohen’s d
effect size for hardness showed that there is an
incremental increase in hardness with UHMWPE
incorporation supports its effectiveness in
enhancing surface durability. Scanning Electron
Microscopy (SEM) revealed a uniform dispersion
of UHMWPE particles within the PMMA matrix at
10% concentration. However, at 20% and 30%
UHMWPE, agglomeration of the particles was
observed, which may have negatively influenced
flexural strength. [Figure 5]



Polymethylmethacrylate (PMMA) remains
one of the most widely employed materials
for provisional restorations in prosthodontics
due to its ease of manipulation, low cost, and
favorable esthetics. Despite these advantages,
its relatively low mechanical strength continues
to
pose a clinical limitation. UHMWPE,
known for its high impact strength and wear
resistance, has been successfully utilized
in composite materials.14 The present study
demonstrated that the addition of UHMWPE
at 10% concentration improved the flexural
strength of PMMA compared to the unmodified
control group. This enhancement aligns with
findings from previous studies by Lee et al.
and Shafiei et al., who reported that moderate
incorporation of polymeric fillers improves the
stress-bearing capacity of dental polymers by
enhancing the load transfer mechanism and
increasing interfacial adhesion between filler
and matrix.15 The increase in flexural strength observed at 10% UHMWPE concentration may
be attributed to effective interfacial bonding
which was evident in the scanning electron
microscopy (SEM) images, which revealed
uniform dispersion of UHMWPE particles
and minimal porosities within the polymer
matrix. This uniformity likely facilitated better
stress distribution across the PMMA-UHMWPE
interface, resembling the characteristics of
semi-interpenetrating polymer networks (SIPNs)
described in polymer reinforcement literature.14-16
The polymer chain entanglement phenomenon
and homogeneous dispersion of filler particles
at
lower concentrations contributed to a
enhanced mechanical interlocking with the
PMMA matrix improving load-bearing efficiency,
cohesive internal structure and reduced weak
points. In contrast, a decline in flexural strength
was observed when UHMWPE concentration
was increased to 20% and 30%. SEM analysis
of these groups exhibited clear signs of filler
agglomeration, leading to non-uniform particle
distribution. Such clustering can create stress
concentration zones, facilitating microcrack
initiation and propagation under load. These
observations are consistent with Yu et al., who
noted that exceeding optimal filler thresholds
can compromise the cohesive integrity of polymer
matrices.17 Moreover, the increased porosity
and voids observed in the high-concentration
groups may be a consequence of mixing and
processing challenges, further undermining the
flexural performance, as reported by Jagger et
al.18 Hence, the findings from this study suggest
that 10% UHMWPE represents an optimal
reinforcement level. Concentrations beyond this
threshold appear to diminish these advantages.
In contrast to flexural strength, Shore A hardness
exhibited a positive correlation with increasing
UHMWPE concentration. All experimental
groups showed higher hardness values than the
control, with the 30% UHMWPE group displaying
the highest values. This consistent increase
suggests that UHMWPE effectively enhances surface rigidity and resistance to indentation,
possibly due to a densification effect driven by
the high crystallinity of UHMWPE. Furthermore,
SEM images of the UHMWPE-modified groups—
particularly at higher concentrations—revealed
smoother and more compact surfaces, which
are indicative of reduced micro-voids and
enhanced surface integrity. These findings are
supported by Wang et al., who emphasized
that polyethylene-based fillers improve wear
resistance and surface hardness in composite
materials.19 Thus, while higher concentrations
of UHMWPE may compromise internal structural
strength, they appear beneficial in enhancing
surface durability. In this study, a self-curing
PMMA resin was employed, which polymerizes at
room temperature and is known to have a lower
degree of conversion compared to heat-cured
resins. This may have contributed to residual
monomer presence, incomplete polymerization,
and shrinkage stresses, which in turn could
have affected filler dispersion and mechanical
integrity. Lima et al. have reported that heat
cured PMMA exhibits superior mechanical
properties due to enhanced polymerization
kinetics and cross-linking density.20
This study addresses a key research gap by
comprehensively evaluating the mechanical
performance of self-cured PMMA reinforced with
varying concentrations of UHMWPE, an area
with limited prior exploration. SEM analysis
further enabled microstructural correlation,
strengthening the validity of mechanical
findings. Importantly, the identification of 10%
UHMWPE as the optimal reinforcement level is
of considerable clinical relevance, particularly
in fabricating long-span or implant-supported
provisional prostheses where both strength and
surface wear resistance are essential.16,18 The
lack of thermocycling and fatigue testing restricts
the results to the extraoral environment, as the
materials are not exposed to thermal fluctuations
and cyclic loading. Future research should
focus on modifying the surface characteristics of UHMWPE, such as through silanization or
plasma treatment, to enhance chemical bonding
with the PMMA matrix. Additional mechanical
tests, such as impact strength, wear resistance,
and bond strength to luting agents, would
provide a more comprehensive evaluation.
Lastly, in vivo or simulated oral condition studies
are warranted to assess biocompatibility and
long-term clinical performance.14,17
From a clinical perspective, the addition of 10%
UHMWPE to PMMA significantly enhances
its
flexural
strength
while maintaining
sufficient surface hardness. This makes it a
promising candidate for long-term provisional
restorations and implant-supported interim
prostheses, particularly in cases requiring
extended functionality. While higher UHMWPE
concentrations further increase hardness, the
accompanying decline in flexural strength
suggests their application may be better suited
to non-load-bearing restorations. Despite these
improvements, UHMWPE-reinforced PMMA
remains a provisional solution and is not a
substitute for definitive restorative materials
such as zirconia or lithium disilicate, which
offer superior fracture toughness and long-term
performance.20
Within the limitations of this study, it is
concluded that: The incorporation of 10%
UHMWPE significantly enhances flexural
strength, making it a promising modification for
durable provisional restorations. An increase in
UHMWPE content to 20% and 30% led to a decline
in flexural strength. A consistent increase in
Shore A hardness was observed with increasing
UHMWPE concentration. The highest hardness
values were recorded with 30% UHMWPE.