Short dental implants offer a reliable alternative to standard-length implants, particularly in areas with limited vertical bone. Traditionally, such cases required bone augmentation, increasing surgical complexity, cost, and morbidity. However, advancements in implant design, surface treatments (e.g., SLActive), and materials like titanium-zirconium (Roxolid) have enhanced osseointegration and primary stability. Biomechanical studies show that occlusal forces are concentrated in the coronal 3 mm of the implant, supporting the effectiveness of shorter implants. Indications include atrophic posterior jaws, proximity to anatomical structures (e.g., sinus, nerve), and avoidance of grafting procedures. Short implants can be used alone or splinted for better load distribution. When placed with proper surgical and prosthetic protocols, they show success rates comparable to longer implants. Thus, short implants provide a minimally invasive, cost-effective, and predictable solution, broadening treatment options in modern implantology.
Key words: short dental implants, atrophic ridge, crestal bone stress, implant biomechanics, bone augmentation alternative.
Short dental implants, defined as those with
a Designed Intrabony Length (DIL) of ≤8 mm
(2006 SSID Conference), have evolved into
a reliable option in implant dentistry (Misch,
2008). Although 7 mm implants have existed
for over 30 years, early designs such as those
from Nobelpharma during the Brånemark era
showed limited success in softer bone (D3/D4),
particularly in the posterior maxilla (Ericsson
et al., 2000). He later noted that eliminating
countersinking improved outcomes, highlighting
the importance of surgical technique (Albrektsson
and Wennerberg, 2004).1 Modern advances
in implant design, surface treatments, and
surgical protocols have significantly improved
the predictability of short implants. They now
demonstrate survival rates comparable to
longer implants, especially in sites with limited
vertical bone height (Esposito et al., 2014).
Their advantages include reduced need for
bone grafting, lower surgical morbidity, shorter
treatment time, and cost-effectiveness (Felice et
al., 2019).2
Short and ultrashort implants are increasingly
used in atrophic jaws, elderly or medically
compromised patients, and select adolescent
cases (Eriksson et al., 2018). This review
highlights their evolution, clinical applications,
outcomes, and limitations, underscoring their
role as a minimally invasive and effective
treatment option in modern implantology.3
The concept of short dental implants evolved
to address clinical challenges associated with
reduced alveolar bone height, aiming to avoid
invasive augmentation procedures (Misch,
2008). Although implants measuring 7.0 mm
or less have been available since the late 20th
century, early adoption was limited due to
biomechanical concerns and variable survival
rates in poor bone quality (Ericsson et al., 2000).4
The scientific history of short implants began
with the development of root-form implants by
Brånemark and colleagues in the 1960s and
1970s. These implants, commercialized by
Nobelpharma, performed well in dense bone
types (D1 and D2) (Brånemark et al., 1977),
showing survival rates of 93.7% in the mandible
and 90.2% in the maxilla. However, significantly
reduced success was observed in the posterior
maxilla, particularly with shorter implants in
softer bone (D3 and D4) (Testori et al., 2004).
In 2006, the State of the Science in Implant
Dentistry (SSID) Conference, organized by
the Academy of Osseointegration, formally
defined short implants as those with a Designed
Intrabony Length (DIL) of 8.0 mm or less, a
definition supported by historical clinical
evidence (Misch, 2008). Implants of 7.0 mm had
already been available for over 30 years, with
6.0 mm and 5.0 mm implants introduced in 1997
and 2008 respectively (Annibali et al., 2012).4
The importance of surgical technique was emphasized during the 2009 AO Annual
Meeting, when Dr. Tomas Albrektsson noted poor
outcomes for 7.0 mm Nobelpharma implants
in the posterior maxilla. However, a study led
by Arun Garg demonstrated that eliminating
countersinking improved implant stability
and survival significantly, with success rates
in the 90% range, underscoring the technique
sensitivity of short implant success (Albrektsson
and Wennerberg, 2004).5
Initially, short implants in the 8–10 mm range were
mainly developed by smaller companies such
as 7br, MegaGen, Bicon, Jeneric, and BTI (Felice
et al., 2019). Over time, major manufacturers
including Straumann, Nobel Biocare, and Astra
Tech began offering scientifically validated short
and ultrashort implants (≤6 mm), demonstrating
survival rates comparable to standard-length
implants when placed under appropriate
conditions (Esposito et al., 2014). Ultrashort
dental implants from different manufacturers
have been designed to address cases with
limited vertical bone height, particularly in the
posterior mandible and maxilla (Eriksson et al.,
2018). These implants range from 5.0 mm to 8.0
mm, with some as short as 5.0 mm qualifying as
“ultrashort.” The Bicon™ implant (6.0 × 5.7 mm)
features a unique plateau-root form enhancing
bone integration, while Astra OsseoSpeed™
and Straumann® implants (e.g., 4.0 × 6.0 mm,
4.1 × 6.0 mm) utilize surface-treated threaded
designs to improve osseointegration and
primary stability. OT Medical OT-F³® implants
are cylindrical (5.0 × 5.0 mm and 4.1 × 5.0 mm),
maximizing bone-to-implant contact in shallow
ridges. The Dentaurum® series offers various
thread patterns within the 5.0 mm length range,
tailored for different bone densities and loading
conditions (Chen et al., 2015).6 These implants
provide a minimally invasive solution in regions
where traditional longer implants are risky or
unfeasible, avoiding complex procedures like
bone grafting or sinus lifts while ensuring long
term stability and function (Felice et al., 2019).
Short and ultrashort implants are indicated
in cases with limited vertical bone height,
avoiding the need for bone grafting. They are
useful for edentulous jaws, single or multiple
tooth replacements, narrow interdental spaces,
adolescent cases (with subcrestal placement),
and atrophic anterior maxillae. Absolute
contraindications include uncontrolled systemic
diseases (e.g., diabetes), recent bisphosphonate
use with ONJ, and recent radiation in the
implant area. Relative contraindications include
heavy smoking, poor oral hygiene, untreated
periodontal disease, and systemic conditions
needing medical clearance. With advancements
in design and surface technology, short implants
now offer high success rates in challenging
conditions.13
Short dental implants, generally defined as those with an intraosseous length of ≤8 mm, have significantly expanded the scope of implant dentistry, especially in cases with compromised vertical bone height. Their use avoids the need for extensive bone grafting procedures, thereby reducing surgical morbidity, cost, and treatment duration. Clinical applications of short implants are diverse and include both partially and fully edentulous patients, with favorable long-term outcomes in various anatomical scenarios.14
In it implant originally featured a turned-surface
finish available in 6.5 mm (“7 mm”) and 9.5 mm
(“10 mm”) lengths since the 1960s. In 1993, an
8.5 mm (actual 8.0 mm) length was introduced
for the 3.75 mm and 4 mm diameter implants.
Both 7 mm and 8.5 mm lengths were later offered
with wide diameter and NobelSpeedy implants.
The Brånemark System implant with a turned
surface finish has been available in 6.5 mm
(“7 mm”) and 9.5 mm (“10 mm”) lengths since
the 1960s. In 1993, an 8.5 mm (actual 8.0 mm)
length was introduced for the 3.75 mm and 4
mm diameter implants. Both the 7 mm and 8.5
mm lengths were also offered in wide-diameter
versions and as part of the NobelSpeedy implant
line. The design features of the self-tapping Mk
III implant, the tapered shapes of the Mk IV
and NobelSpeedy implants, and the conical
connection abutment interface were integrated
to create the NobelParallel CC implant.21
Straumann introduced 6 mm short implants
with the TPS surface in the late 1980s, showing
favorable clinical results by the late 1990s. In
1998, the SLA (Sandblasted Large-Grit Acid
etched) surface was launched for 6 mm implants,
followed by the SLActive surface in 2005. The
SLActive surface improves osseointegration speed and bone-to-implant contact, while
the SLA surface remains one of the most well
documented in the market. Later, the Roxolid
alloy (TiZi) was introduced, enhancing implant
strength and osseointegration, initially focusing
on reduced diameter implants. This alloy is
now used across Straumann’s implant range,
including SLA and SLActive surfaces.
The 6 mm implants come in Standard (2.8 mm
polished collar) and Standard Plus (1.8 mm
polished collar) designs, with body diameters
of 4.1 mm and 4.8 mm, and neck widths of 4.8
mm (regular) and 6.5 mm (wide). The implant
has a solid screw parallel-wall body with 1.25
mm thread pitch and a rounded apex. The
tulip-shaped neck improves primary stability,
especially in the posterior maxilla. (Fig.1)

The polished collar is positioned at the soft tissue
level, reducing crestal bone loss and enhancing
peri-implant tissue stability. Since these implants
are mostly used in posterior regions, esthetics are
less critical, and the polished collar’s benefits outweigh its slight visibility (Figure 1). The
tissue level design includes an internal Morse
taper conical connection (SynOcta), providing a
biological seal and strong mechanical stability,
which is especially helpful for short implants by
reducing the crown-to-implant ratio.
Short implants are an effective, minimally
invasive alternative for atrophic posterior
maxilla cases, reducing morbidity, treatment
time, and cost compared to sinus floor elevation
(SFE). Patient satisfaction is high.22 However,
short implants should be splinted when placed
as multiple adjacent implants in the posterior
maxilla for better outcomes. Single short implants
in molar sites are generally not recommended
except in rare cases like elderly patients with low
bite force.
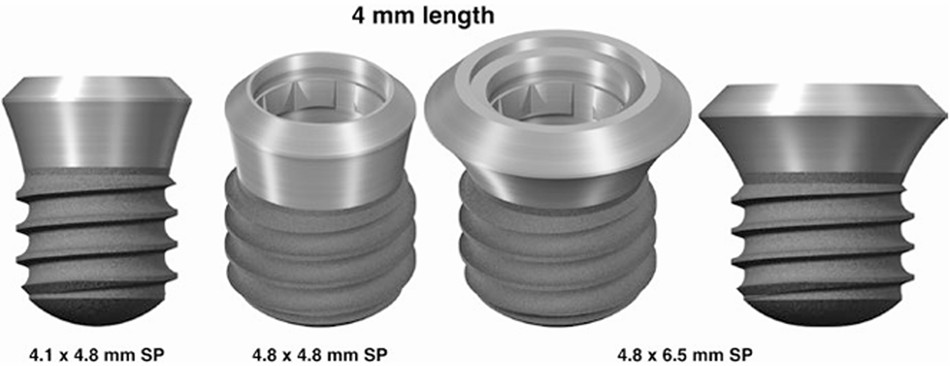
The 4 mm long, solid screw, SLActive soft tissue level implant with a 0.8 mm thread pitch and titanium grade 4 was introduced in 2009, differing from the well-known 6 mm implant. Unlike the 6 mm implant’s 1.25 mm thread pitch, this shorter implant features a finer 0.8 mm pitch. It is available only in Roxolid (Titanium Zirconium alloy) with an SLActive surface and a Standard Plus (SP) 1.8 mm polished collar neck. It comes in three configurations (Figure 2):
The surgical protocol is similar, with drills and
depth gauges marked at 4 mm. Extreme care
must be taken to avoid overdrilling both vertically
and horizontally, as this risks nerve damage or
loss of primary stability. In the atrophic posterior
mandible, where alveolar bone is often resorbed,
implants are placed in cortical bone. The
reduced thread pitch provides very high primary
stability, so tapping is strongly recommended to
prevent excessive insertion torque, which could
compromise osseointegration.23
Many Studies have shown that the short- and
long-term survival rates of ultrashort (5–6
mm) wide plateau root form implants in the
posterior maxilla are comparable to those of
longer implants. While conventional protocols
recommend longer implants that often require
extensive bone grafting, recent clinical evidence
suggests that ultrashort plateau-type implants
can successfully restore maxillary molars
without the need for large grafts. This challenges
the traditional belief that ultrashort implants
provide insufficient bone contact to withstand
masticatory forces, particularly in the poorly
mineralized maxillary bone.24
In clinical practice, 5mm and 6mm plateau
implants have demonstrated reliable long-term
outcomes, avoiding the complications and costs
associated with extensive grafting. Therefore, the
use of ultrashort plateau implants with minimal
or no grafting presents a predictable and less
invasive alternative to longer implants with large
grafts in the posterior maxilla.25
Ultrashort implants (≤6 mm) have shown
excellent long-term performance in the posterior
mandible, where bone density is typically
high. Despite earlier concerns, studies have
demonstrated that these implants provide stable osseointegration and maintain crestal bone
levels for over a decade. Their use reduces the
risk of complications such as nerve injury and
eliminates the need for bone grafting in many
cases. With advances in implant design and
surface technology, ultrashort implants now
offer a reliable, minimally invasive solution for restoring posterior mandibular teeth, with
survival rates comparable to longer implants.26
The development of short dental implants
(≤8 mm) marks a significant advancement in
implant dentistry, offering solutions for cases
with limited vertical bone height without the need
for invasive grafting procedures. Initially met
with skepticism due to concerns over reduced
stability and higher failure rates—especially in
poor-quality bone like the posterior maxilla—
modern short implants have demonstrated
survival rates comparable to standard implants,
thanks to advances in design and surface
technology.27 Standardization of short implants
following the 2006 SSID Conference, along with
innovations such as plateau-root forms, SLA/
SLActive surfaces, and high-strength alloys like
Roxolid, has enhanced bone-to-implant contact
and load distribution. These features improve
primary stability, reduce stress on crestal bone,
and mitigate crown-to-implant ratio concerns.28
Clinically, short implants are highly beneficial in
challenging situations, including atrophic ridges,
elderly or medically compromised patients, and
full-arch restorations. Their minimally invasive
nature reduces surgical time, cost, and patient
morbidity. However, success depends on careful
case selection, proper surgical technique,
implant design, and appropriate loading
protocols. Splinting short implants, especially in
the posterior maxilla, improves outcomes, while
single molar short implants require cautious
planning.29 Long-term studies now support the
use of short and ultrashort implants (≤6 mm),
showing comparable survival rates to longer
implants. This challenges traditional views and
expands treatment possibilities for anatomically
limited cases.30 Short dental implants have
transitioned from a less reliable option to a
well-supported, effective treatment modality.
When used judiciously, they offer predictable,
minimally invasive, and cost-effective solutions
that
enhance both function and patient
satisfaction.31
Short dental implants have emerged as a
viable alternative to conventional implants in
cases with reduced vertical bone availability,
offering predictable outcomes with minimal
surgical morbidity. Advances in implant macro-
and micro-design, surface modifications, and
improved biomechanical understanding have
enhanced their long-term clinical performance.
Current evidence indicates comparable survival
rates to standard-length implants while reducing
the need for complex bone augmentation
procedures. Nevertheless, their success is
highly dependent on meticulous case selection,
prosthetic planning, and controlled loading
conditions. As ongoing research further optimizes
implant design and protocols, short implants are
poised to play an increasingly prominent role in
contemporary implant dentistry.