Immediate implant placement in the anterior maxilla presents both an opportunity and a challenge due to high aesthetic demands and anatomical limitations. This case report describes the clinical management of a patient requiring tooth extraction and immediate implant placement in the aesthetic zone. Atraumatic extraction was performed to preserve the alveolar bone, followed by precise implant placement. Particular attention was given to the soft tissue architecture and buccal bone integrity to optimize aesthetic outcomes. The case demonstrates the importance of proper case selection, surgical technique, and prosthetic planning in achieving predictable functional and aesthetic success. Follow up over 12 months showed stable peri-implant tissues and satisfactory patient-centered results, highlighting the viability of immediate implantation in carefully selected cases within the aesthetic zone.
Key words: Immediate implant placement, aesthetic zone, Implant aesthetics, Socket preservation, Atraumatic extraction.
Dental implants are a well-established solution
for the replacement of missing teeth, offering
long-term functional and aesthetic benefits.
Immediate implant placement—defined as
implant insertion at the time of tooth extraction—
has become increasingly popular due to its
advantages in reducing overall treatment time,
preserving alveolar bone, and maintaining soft
tissue contours.
In the anterior maxilla, also known as the
aesthetic zone, immediate implant placement
presents specific clinical challenges. The thin
buccal bone plate, high aesthetic demands,
and risk of soft tissue recession require careful
planning and precise surgical technique. To
mitigate the risk of ridge resorption and to
enhance peri-implant tissue stability, bone
grafting is often employed, particularly in cases
where a gap exists between the implant and the
socket walls.
This case report describes the immediate
placement of a dental implant in the anterior maxilla following atraumatic tooth extraction,
combined with bone grafting to support the
buccal contour and enhance aesthetic outcomes.
A 28-year-old male patient reported to the
Department of Prosthodontics and Crown &
Bridge with a chief complaint of a fractured upper
front tooth numbered 21 with the desire for a
fixed replacement. The patient was systemically
healthy, a non-smoker, and had no significant
medical history. Clinical and radiographic
examinations revealed a non-restorable fracture
of tooth 21 with intact surrounding soft tissue
and adequate alveolar bone volume and with no
signs of infection or pathology at fractured site.
(Fig. 1)
After a thorough discussion of the available
treatment options, including the advantages and limitations of immediate implant placement, the
patient consented to undergo extraction of tooth
21 followed by immediate implant placement
and bone grafting.

Under local anesthesia, tooth 21 was
atraumatically extracted using periotomes to
preserve the integrity of the alveolar socket,
particularly the buccal bone plate. (Fig. 2 and
Fig. 3). The socket was carefully debrided and
irrigated. A dental implant with dimension of
4.2 mm × 13 mm titanium implant (Norris) was
placed in a palatal position within the socket
to achieve optimal primary stability and a
prosthetically driven position. (Fig. 4 and Fig.
5). An insertion torque of 35 Ncm was achieved,
confirming satisfactory primary stability. A gap
of 2 mm was noted between the buccal aspect of
the implant and the socket wall. To promote bone regeneration and preserve the ridge contour,
the gap was filled with a bone graft (Nova
bone). A healing abutment was placed, and the
site was sutured with 4-0 resorbable sutures.
(Fig. 6 and Fig. 7) The patient was prescribed
antibiotics and analgesics and advised to
follow standard postoperative care instructions.
Follow-up evaluations at 1 week, 1 month, and
3 months showed uneventful healing with no
signs of infection or soft tissue complications. At
3 months post-placement, radiographic evaluate
on showed good integration of the implant and
evidence of bone fill around the grafted area.
(Fig. 8 and Fig. 9)
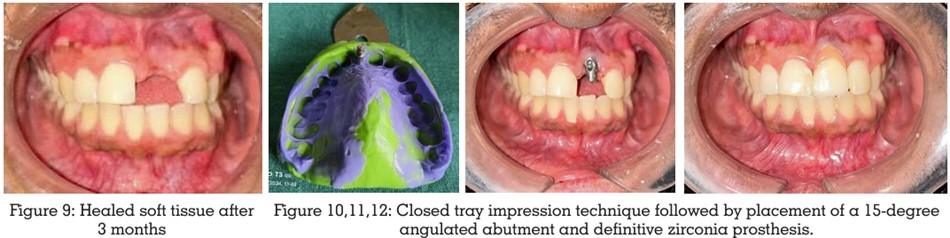
After confirming successful osseointegration,
a Cement-retained provisional crown was
delivered to guide the soft tissue healing and
shape the emergence profile. The patient was
monitored for an additional 6 weeks, during which
excellent soft tissue adaptation and aesthetic
outcomes were observed. Subsequently, a
definitive zirconia crown was fabricated and
delivered. The final prosthesis demonstrated
excellent shade matching and harmonious
integration with adjacent teeth. (Fig.10, Fig.11
and Fig.12)
Immediate implant placement is indicated
in cases of tooth extraction due to trauma,
root fracture, root perforation, root resorption,
unfavourable crown: root ratio and with no dehiscence or fenestration defect1
Contraindications include site with active
infection, insufficient bone apical to tooth
socket apex (<3mm) and wide or long gingival
recession2. In general, approximately 5% of
implants are expected to be lost regardless the
protocol being used. The success rate in maxilla
has been stated as 66-95.5% and in mandible is
90–100%4. No statistically significant differences
in mean crestal bone loss and mean probing
pocket depth between the protocols was found.
Immediate implant placement was initially said
to preserve alveolar bone. However this is said
to be controversial since morphologic changes
of the post-extraction site may occur despite
immediate ⁄ early implant placement. Buccal
wall of socket being thin, slightly palatal ⁄ lingual
placement of the implant in the extraction
socket is recommended to avoid exposure of
the implant surface. And also for preservation
of bone, careful extraction is recommendable
and it is advised to section multi-rooted teeth
before removal3. Controversies exist on whether
local pathology has an adverse effect on the
outcome. Chronic infection is not an absolute
contraindication
for
immediately placed
implants, however, thorough debridement of the
alveolus should be made. The use of antibiotics
prophylactically, is recommended in medically
compromised patients. In the present study
no local pathology was present3. Small gaps
between implant surface and socket wall have
a potential for spontaneous healing. GBR and grafting perform successfully for augmentation
of dehiscences and fenestrations; however, no
evidence exists that one technique or material
is superior to others. In the present study, no
osseous defect had warranted the use of any
graft material5.
Immediate implant placement in the aesthetic
zone offers significant advantages, including
reduced treatment time, preservation of alveolar
bone, and maintenance of soft tissue contours.
However, its success depends on careful case
selection, atraumatic extraction, proper implant
positioning, and appropriate use of grafting
materials when needed. In the present case,
the use of a bone graft in conjunction with
immediate implant placement contributed to
the preservation of the buccal contour and
supported an optimal aesthetic outcome. The
clinical and radiographic results observed
during follow-up indicate that, when executed with precision, immediate implant placement
with adjunctive grafting can be a predictable
and effective treatment modality for replacing
teeth in the anterior maxilla. Continued follow
up is essential to monitor long-term stability
and ensure sustained aesthetic and functional
success.