Obturator is given for patient with maxillary defect which occurred either due to trauma or congenitally. They are generally classified into three that is immediate, interim and definitive obturator. Immediate obturator is the type of obturator that is given immediately after surgery. Fabrication of this type of obturator is done on pre-surgical cast. It is a base plate type of obturator. Interim obturator is the obturator given after surgery and before proper healing. This case report deals with the fabrication of definitive obturator, an obturator that is given after proper healing. Fabrication of obturator can be done in different ways. They differ in the mode of acrylisation. Acrylisation can be done by two methods, single piece and two piece type of Acrylisation. This case report describes the use of two piece type of acrylisation by lost salt technique.
Key words: Palatal Obturator, Congenital Defect, Acquired Defect, Prosthesis, Cystectomy.
The term obturator has its origin from a Latin
verb “obturare” which means to close or to
shut off. Boucher in 1982 defined obturator
as a prosthesis used to close a congenital or
an acquired opening in the palate. According
to GPT 9, Obturator is defined as prosthesis
used to close a congenital or an acquired
tissue opening, primarily of hard palate and
or contiguous alveolar structures.
Ambroise Pare was the first person to use an
obturator in the year 1541. He used it for closing
a perforation of the hard palate. Sir Pierre
Fouchard, father of scientific dentistry, described
two types of palatal obturators in 1728. First type
had wings in the form of propellers whereas
the second type had retaining feature in the
form of butterfly wings. These wings could be
folded together while being inserted and could
be spread out with a special key after insertion.
William Morton in 1869 treated palatal defect
with a gold plate to which missing teeth were
soldered.1
Primitive man used wood, cotton, gum or stone
to close a defect. However, the material of
choice in today’s scenario is polymeric in
nature. These include vinyl chloride polymer
and copolymers, acrylic types and silicone
rubbers, among which the silicone rubbers
are mostly used.
Functions of an obturator are beyond
imagination. They play a major role in increasing
the confidence of an individual by reshaping
and reconstructing the defect. They aid in
keeping the wound and defective area clean
and enhance the healing of traumatic or
post surgical defects. They play a vital role in
improving the speech or at some instances by
making speech itself possible. Lip and cheek
positions are often corrected by an obturator.
They help in improving the impaired mastication
and deglutition functions. Flow of exudates into mouth is often reduced by an obturator. They
even act as a stent to hold dressing or packs
post surgically2.
There are mainly three types of obturator;
surgical, intermediate and definitive obturator. They
are classified based on the time of fabrication.
Surgical obturator is given immediately after
the surgery. Intermediate obturator is given two
weeks after resection and definitive obturator
is given after complete healing of mucosa and
other oral structures.3,4
Now a days, technology has evolved so
well which enables better use of obturators.
Stereophotogrammetry enables the soft tissue
analysis. CBCT and MRI has their role in advancing
the procedures. Thus technology plays its own role
and make the clinical works a little easier.
A 40 year old female patient reported to
the department of Prosthodontics and Crown
& Bridge with left maxillary defect. She had
undergone maxillectomy 4 years back due to
squamous carcinoma. She had a large defect of
size 3 cm length 2 c m broad and 4 cm depth and
defect will come under type 1 Aramany defect
(fig1). Intra orally patient had the following
missing teeth: 13 14 16 17 22 23 24 25 26 27
35 36 46 47 and 43 44 45 were root canal
treated teeth. Since high end treatment such
as implant supported prosthesis or cast partial
obturator were not feasible for the patient due
to their economic status, a conventional acrylic
obturator on upper arch and acrylic RPD and joint crown irt to 43 44 and 45 in lower arch
were planned as treatment.
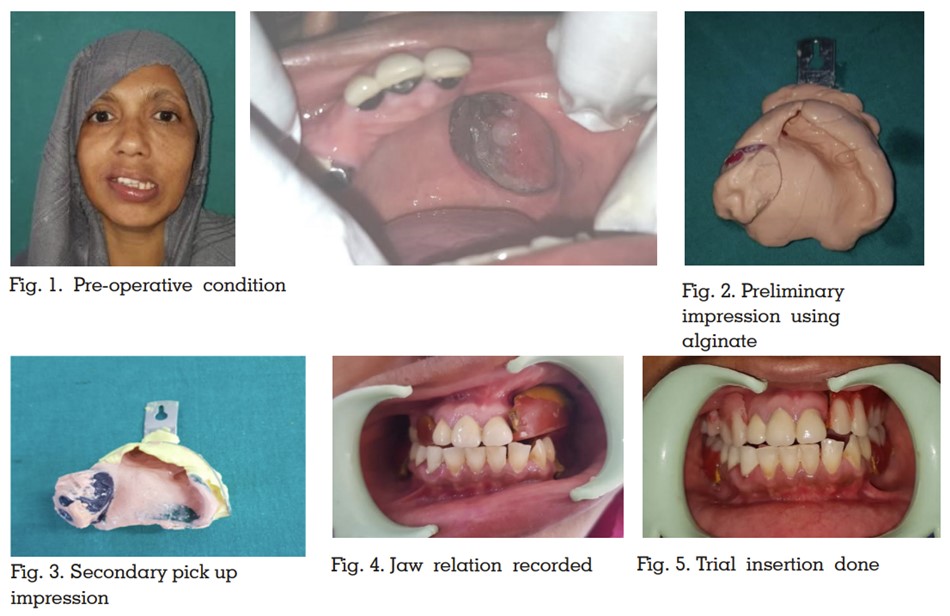
Maxillary and mandibular preliminary impression
was made using alginate (Fig.2). Impression was
poured with dental stone and custom tray was
fabricated on the upper arch. Using this custom
tray border moulding and posterior palatal
seal area was recorded. Impression compound
was then used to record the defective area of
maxilla. Secondary impression was recorded
using alginate as it helps in easy removal
of impression from the undercut of defective
area (Fig 3). Secondary cast was poured using
dental stone.
Cast was duplicated using agar agar and kept,
shellac base plate was adapted on master cast
and occlusion rim was fabricated. Jaw relation
was recorded (Fig 4) and transferred to mean
value articulator and then teeth arrangement
was done. A clinical trial insertion was done
(Fig 5).
Until now, the laboratory procedures for the
fabrication of a complete denture and an
obturator remain the same. The difference
lies in the acrylisation procedure.
Retentive clasp is fabricated using orthodontic
wire on the abutment as it enables easy insertion
and removal without compromising the retentive
features.
Waxing up, investing and dewaxing of the
trial denture was done. In the mean time wax
is adapted on the roof of the defective area on
the previously duplicated cast and is acrylised in
another flask for fabrication roof of the bulb (Fig 6).
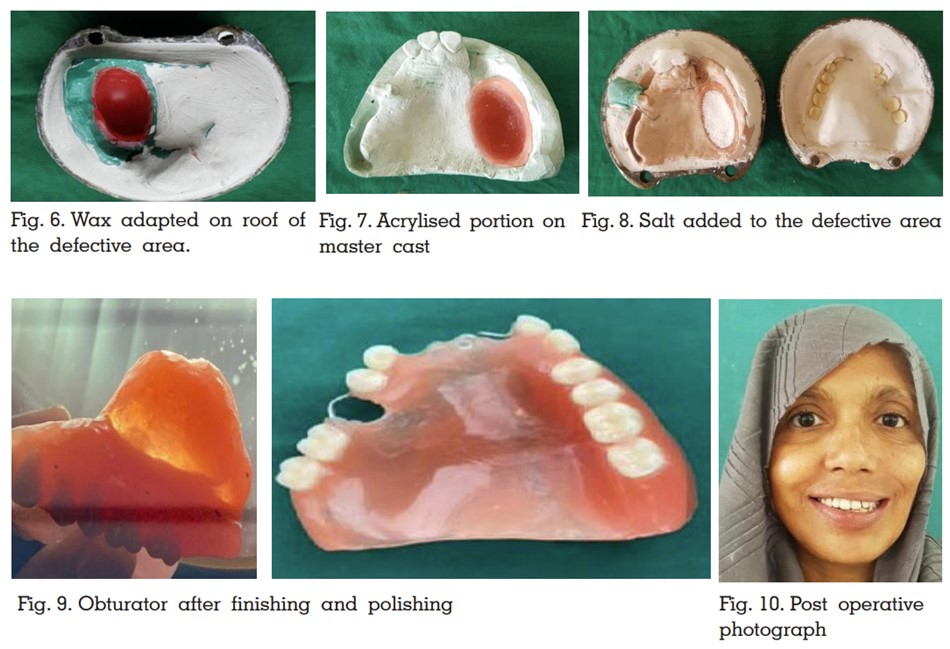
The acrylised portion will act as the roof of
hollow bulb obturator and this was then placed
in the defective area of the dewaxed master
cast. Then salt was filled into the acrylised
portion (Fig 8) and Acrylisation was done as
usual.
After retrieval of the acrylised portion, a small
hole was put on the intagilio surface In bulbous
portion of the obturator and salt was removed
by injecting water into it. Once the salt was
completely removed, the hole was closed by auto
polymerised acrylic resin. Finishing polishing
was done. Final insertion of the obturator was
done(fig 9).
A palatal defect which may be congenital or
acquired is of great concern as it affects speech,
mastication, and deglutition and to a great
extent, aesthetics. They can be prosthetically
rehabilitated by an obturator. Fabrication of obturator and its retention and stability while
placed In mouth is really important.5
The weight
of the obturator is one of the main reasons
for the dislodgement of obturator. Thus making
it light will enhance the stability.6
Obturators
can be given at three different stages and are
named accordingly as immediate, surgical and
definitive obturators.7,8 A surgical obturator is
given during surgical phase. It can be immediate
surgical obturator or delayed surgical obturator.
An immediate surgical obturator is inserted at
the time of surgery whereas a delayed surgical
obturator is inserted when another surgery is
to be carried out 1-2 weeks after the removal
of the defect. This obturator can be given either
for partially or totally edentulous patients. No
teeth will be present on the obturator. During
healing phase, an interim obturator is given. They
are given to make sure that the wound contraction
is minimized and ideally advised after 3-4 weeks
of surgery. They can also be immediate or
delayed. Immediate interim obturator can be
modified from an immediate surgical obturator,
by adding teeth and bulb relined with tissue
conditioner onto it. When other procedures like
radiation or improvement in mastication or
deglutition is to be carried out, an interim
obturator is given at a later stage and is
called delayed interim obturator. A definitive
obturator is given at the healed phase when
the surgical wound is completely healed. Prior to
the placement of a definitive obturator, thorough
examination of the oral cavity is to be done. All
the carious teeth should be restored; those with
poor prognosis should be carefully extracted,
keeping in mind regarding osteoradionecrosis.4
Patients diagnosed with large cystic defects
usually undergo enucleation or marsupialisation.
Post marsupialisation, bone defects are quite
common and mostly results in clot dislodgement
and improper healing. In such scenario, obturator
turns out to be the best choice as they stabilize the
defective area and aid in easy recovery. Mostly a
partial acrylic denture obturator is used in restoring function and aesthetics.
Design of the obturator depends on the defect
and the classification to which it belong.
Minimizing the weight of the prosthesis was
essential and various techniques were employed.
This included ice incorporation salt technique
and sugar technique, use of thermoplastic
method to get hollow bulb.9,10 The disadvantage
of ice and salt/ sugar technique is the
tendency of distortion of the shape due to
pressure applied during packing.
Obturator has been used for prosthetic
rehabilitation from early 16th century. As years
roll down, the material of choice may differ,
the methods of fabrication get advanced, and
the ease and convenience of use get improved.
The defect differs from person to person and so
is the design of the obturator. Various designs
were put forward and it is the clinician who
should choose them wisely and make it more
user friendly for the patient.