Trismus is a condition commonly encountered by the dentists, causing limited mouth opening, interferes with oral hygiene, restricts access for dental procedures, and may adversely affect speech and facial appearance. The overall success of treatment depends on prompt recognition of the cause and initiation of appropriate management. Ideally trismus appliances are used in conjunction with physical therapy effectively for the management of Trismus due to muscle fibrosis or scar tissue that has not yet matured. Currently several trismus appliances either externally activated or internally activated are available commercially. This case report presents a simple and cost-effective approach for the management of Trismus using a Threaded Tapered Screw appliance.
Key words: Trismus, Tapered Screw Appliance, Mouth Opening
Trismus refers to a motor disturbance of the
trigeminal nerve especially sustained prolonged
tonic contraction of the masticatory muscles
causing limited mouth opening.1
The word
“Trismus” is derived from the Greek word “Trismos
or Trigmos” which means grinding or rasping or
gnashing2
. However in layman terms Trismus
denotes limitation of mouth opening due to reduced
mandibular mobility3
. The prevalence of trismus
ranges from 5% to 38%.4
At maximum mouth opening normal interincisal
distance varies from 40–45 mm. The maximum
mouth opening in dentulous patients is measured
between the incisal edges of maxillary and
mandibular central incisors and in edentulous
patients between the maxillary and mandibular
alveolar ridges. Since the width of the index
finger at the nail bed is between 17 and 19 mm,
two fingers’ breadth (40 mm) up to three fingers’ breadth (54–57mm) is considered as normal width
of mouth opening.5
Diagnosis of trismus is made when maximum
interincisal distance (MID) is less than 40–45 mm.6
Based on the range of mouth opening Trismus can
be classified as Light trismus(Mouth opening of
> 30 mm), Moderate trismus (Mouth opening of
15-30mm) and Severe trismus(Mouth opening of
< 15 mm).7
Various pathosis that leads to trismus are
congenital disorders, infections, trauma,
iatrogenic, neoplasia, radiotherapy, chemotherapy,
temporomandibular disorders, drug induced,
psychogenic, oral submucous fibrosis.8
Depending on the cause various treatment
modalities were postulated and tried. Trismus
resulted because of muscle fibrosis / formation of
immature scar tissue, can be managed judiciously
with physical therapy and use of trismus appliance.
However, trismus resulted due to intracapsular
anomalies involving temporomandibular joint, bony interference from styloid or coronoid processes,
formation of dense fibrosis may require surgical
interventions. The design of a device for jaw motion
rehabilitation should provide wide range of mouth
opening, adjustable maximum force applied to the
jaw, sustained and constant stretch at the desired
range of motion; ease of use by the patient him/
herself for the entire exercise session, periodic
repetition of the exercise at invariant conditions
and in non-cooperating patients with reduced
muscle force.9
Trismus patients may experience a marked
restriction of jaw movements which can hamper
overall physical and mental health of the patient.
This article describes management of post
traumatic trismus using threaded tapered Screw
appliance.
A 20yr old male patient referred to the department
of prosthodontics Government Dental College, Alapuzha for the management of restricted mouth
opening. Patient revealed a history of fracture
dislocation of left condylar process of the mandible
due to Road Traffic Accident (RTA) occurred 1month
back which was managed conservatively.
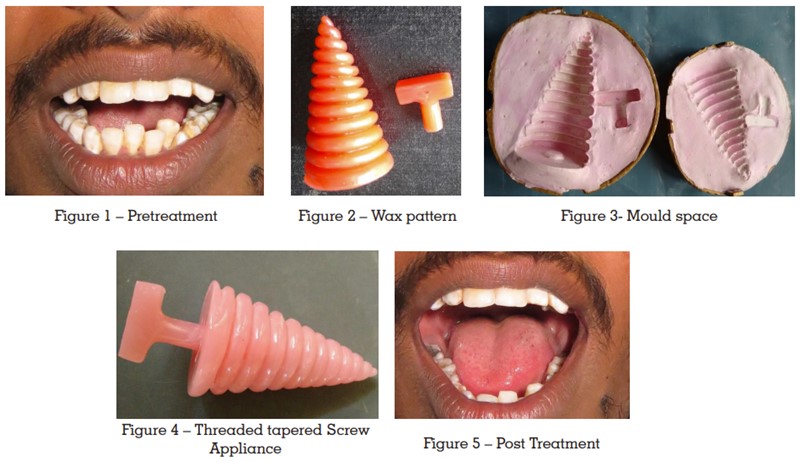
Extraoral examination revealed tenderness
and clicking sound present on the left
Temperomandibular Joint (TMJ), mouth opening
of about 25mm, deviation of mandible towards
left side on mouth opening.(Fig 1) Intraoral
examination revealed the presence of full
complement of teeth. Radiographic examination
comprised of orthopantamograph and computed
tomography which revealed dislocation fracture
of left condylar head and obliteration of left TMJ
space.
Based on the clinical and radiographic findings it
was diagnosed to have early fibrous ankylosis of
left TMJ. Following comprehensive diagnosis, it was
planned to manage by immediate non invasive,
non surgical approach mainly physiotherapy with
threaded tapered screw appliance.
The appliance was fabricated using conventional
compression moulding technique. A wax pattern
of the appliance and T shaped handle was carved
in modeling wax. Modelling wax was shaped
in the form of a cone, serrations were marked
with the help of a thread and it was deepened
using a carver to obtain the wax pattern of the
appliance.(Fig 2) An appropriate dental flask
with sufficient clearance was selected. Plaster
of paris was mixed in the right proportion and
poured into the lid and middle of the flask. A
layer of plaster of paris was applied around the
carved wax pattern to avoid air bubbles. Place
and press the wax pattern and handle into the
centre of the flask. Care should be taken not to
create any undercuts. Remove the excess plaster
and fill the deficient areas before the initial set
of plaster. Smoothen the surface of plaster with a
piece of cotton followed by emery paper after its
initial set. Apply separating medium all over the plaster surface except over the wax. A proper mix
of plaster of paris was poured into the base of the
flask. The base of flask was kept into position and
checked for complete seating. All the excess plaster
of paris is removed from the flask and place the
flask assembly in a dental clamp, tighten it and
allow the material to set for 30 min. Dewaxing
was done to get the mould space (Fig3). A single
coat of separating medium is applied on all the
plaster surface. Autopolymerising acrylic resin
mixed in dough state was packed into the mould
space. A wet cellophane sheet was placed over
the resin dough and keep the second half of the
flask over the cellophane sheet. Compress the flask
in a hydraulic bench press at 1500 psi pressure.
Remove the excess flash using a blunt knife, After
the final closure, flask is left under pressure of 3500
psi for 3hrs to ensure complete polymerization.
On completion of curing the appliance and T
shaped handle was retrieved carefully, finished
and polished. Handle is attached to the base of
the appliance using autopolymerising acrylic resin
and final polishing was done.(Fig4)
The appliance was delivered to the patient.
He was advised to place the smaller end of
the tapered screw appliance between upper
and lower premolars and rotate the appliance
clockwise using the handle. This rotation made
the appliance push more lingually resulting in
stretching effect of muscles and gradual increase
in mouth opening. The patient was instructed
to perform this exercise 6 to 7 times daily. Each
session should be done for 5minutes initially and
increased gradually by 2 minutes per sitting upto
20minutes. Stretch should be hold for 10 seconds,
rest for 10seconds and again repeat. Patient was
also motivated to do massage, alternate warm
and cold fomentation, jaw opening, closing and
side to side jaw movement exercises.
Patient was advised to continue the exercise for a
period of 6 months at regular 2 weeks of review. At
each recall visits prognosis and difficulties during
the exercises were evaluated and instructions were given to motivate the patient.
Mouth opening was improved to 34 mm after
2weeks and 45mm after 1 month (Fig 5). It was
also noted that deviation of mandible on mouth
opening was also reduced during recall visits.
A fracture dislocation of the condylar head can
result in a mechanical obstruction and limited jaw
function.10 A detailed history, clinical, functional
and radiographic examination facilitating correct
diagnosis followed by immediate physiotherapy
yields a drastic improvement in mouth opening.
Depending on the cause various measures have
been utilized to counteract trismus. Treatment
objectives are to remove edema, soften and stretch
the fibrous tissue, improve muscular strength,
restore circulatory efficiency, thus increasing
mouth opening, and retain muscular dexterity.
Treatment plan should ideally be directed towards
managing the cause of trismus. Literature review
demonstrated the efficacy of different trismus
appliances to improve the mouth opening.11
Studies have proven that sledge-hammer, tied
to the mandible for 2 min twice a day, and an
orthodontic “clothes pin appliance” inserted
between the molars resulted an increase in mouth
opening of 18mm and 6 mm respectively.12 Trismus
appliances impart force either in continuous or
intermittent manner, light or heavy, and elastic
or inelastic13. They includes Dynamic bite opener,
Threaded tapered screw, Screw type mouth
gag, Tongue blades, Continuous dynamic jaw
extension apparatus. Based on their design trismus
appliances can be either externally activated
or internally activated appliances. Externally
activated appliances utilized stretching the
elevator muscles by depressing the mandible
to increase mouth opening, Internally activated
appliances rely on patients depressor muscles to
stretch the elevator muscles. It was proved that
elevator muscles generate 10 times greater force than those generated by the depressor muscles.
The amount of force delivered depends on the
strength and motivation of the patient.10
The present case was managed with a threaded,
tapered screw made of acrylic resin. The threads
guides the teeth along the increasing taper
and the patient controls the timing and degree
of pressure required to gradually increase the
jaw separation. This method is simple and cost
effective as compared to other methods and it was
easy for the patient to use. The threaded tapered
acrylic screw functions on the patient’s depressor
group of muscles to separate the jaws. Patient
motivation is the key factor in the success of this
kind of appliance. The patient was recalled every
2 weeks to evaluate the improvement in mouth
opening. At each recall visits patient was instructed
that pain during the stretch was normal and was
motivated to continue the exercise for further
improvement in mouth opening. The force imparted
by this appliance is in elastic, and its direction
is limited by the mechanical pressure available
between the posterior teeth. Unfortunately use of
this appliance is restricted to dentate or partially
edentulous patients and anterior teeth in particular
can become loosened if excessive force is applied
during its use.14
Trismus is usually a secondary sign of any TMJ
pathology and is mostly harmless. Any pathology
that restricts mouth opening carries a mental
stigma to the patient. Hence prompt diagnosis
and initiation of appropriate management yields a
drastic improvement in mouth opening helping to
restore the physical, psychological, and emotional
health of the patient.