Modern dentistry changed tremendously with implant surgery. For a successful implant therapy a proper diagnosis and treatment plans is required. Teeth loss may be due to physiological as well as pathological factors are common. The complete loss of teeth causes various problems like difficulty in mastication, improper phonetics, and unacceptable esthetics of patients. Implant supported prosthesis give the dentist an opportunity to restore normal function and esthetics. Successful osseointegration enables dentist and patient to accept a full arch dental prosthesis.
Key words: Implant supported fixed prosthesis, Metal Coping, Bisque trial
The objective of a dental prosthesis is the
replacement of teeth and its associated tissues
to restore form, function and esthetics. Oral
rehabilitation of patients with fully or partially
edentulous patients are always a challenge to
the prosthodontist1
. The dental implant is the
most charming modern treatment modality in dental practice because it fulfills the requirement
of retention, stability, support, comfort, contour, and
esthetic. The increased success rate of implant-supported prostheses has also increased the
esthetic demands of patients.2
Advances in dental implant research, design and
their clinical application have greatly changed
dental care. Improved protocols in implant
therapy over the last several decades have made
implant supported restorations biologically and
mechanically predictable. Full arch implant-supported restorations are increasingly popular,
but many patients are not psychologically ready
for the extractions and alveolectomy that is
often required. The following case presentation
demonstrates the combined use of dental implants
and tooth supported fixed dental prostheses to
restore the patient’s esthetics and function.
A 56 year old female patient reported to Department
of Prosthodontics, Government dental college,
Trivandrum with a chief complain of an ill-fitted
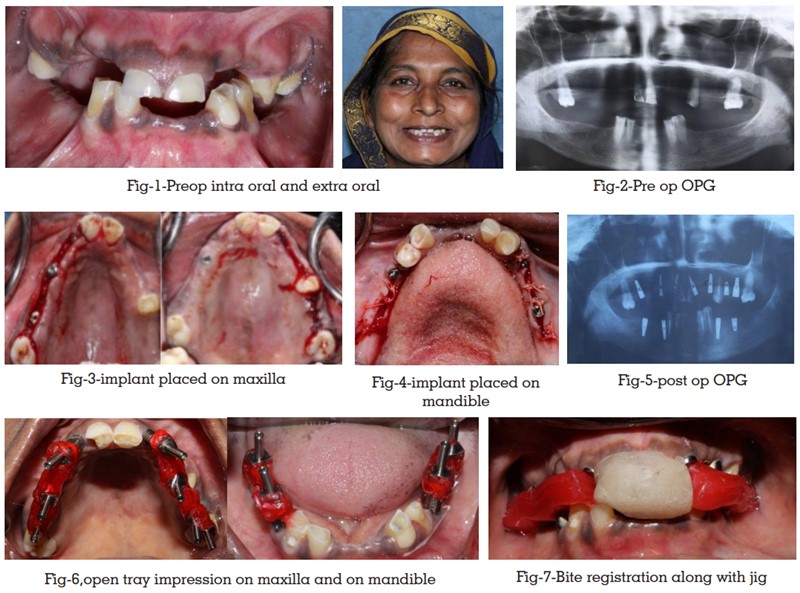
partial denture in both the arches. A completed case history was taken followed by a thorough intra oral
examination. On intraoral examination, the patient
had partially edentulous upper and lower arch.
Teeth present were 11, 21, 15, 18, 28, 32,33,43,44.
Attrition was present on 11,21,32,33,43,44. (Fig.
1) The natural teeth present were periodontally
sound. No relevant medical history. Past dental
history revealed the extraction of multiple teeth
due to dental caries.
The patient was advised for root canal treatment
of natural teeth except 18 and 28. Patient was
also advised for Orthopantomography (OPG)
(Fig. 2) and Cone beam computer tomography (CBCT) of the maxillary and mandibular arch. After
evaluating the radiographs, it was concluded that
there was a good amount of bone height, bone
width, bone density, and adequate inter-arch
space. Hence, the treatment plan was decided as
an implant-supported fixed prosthesis.
Patient consent was taken prior to surgery. 2
stage surgical protocol was planned. Patient was
instructed to have antibiotics prior to surgery.
After radiographic analysis of CBCT and OPG
it was decided to place seven implant in the
maxillary arch with 12, 14, 16,17, 22, 24 and 27
positions and four implants in the mandibular arch
with 34, 36, 45, 47 and positions respectively. The surgical procedure was planned in two phases. In
the first phase of treatment, the surgical placement
of seven maxillary implants of dimensions 3.5×13
mm, 3.5×13mm, 4.2×11.5mm, 3.5×13mm,
3.75×11.5mm, 4.2×11.5 mm respectively (Fig. 3)
and for mandibular arch, surgical placement of
four mandibular implants of dimension 3.5×10mm,
3.75×8,3.5×10mm, 3.75×8mm respectively (Fig. 4)
were planned. Mucoperiosteal flap was elevated
all over the maxilla, Implants were placed followed by placement of the cover screws and suturing was
done. Postoperative care include administration
with antibiotics, analgesics, and mouthwash.
Maintenance of oral hygiene and ice pack if
needed was suggested. Similar procedure was
followed for mandibular arch and suturing was
carried out. A post operative OPG was advised
(Fig.5). After 4 months, patient was recalled and
postoperative OPG was made and checked for proper osseointegration. After confirming
osseointegration, flap was elevated and cover
screws were removed and healing abutment was
placed and waited for three weeks for healing to
take place.
After the three weeks of second-stage surgery, the
steps for definite prosthesis were commenced,
healing abutments were removed. Since the patient
had a collapsed bite, it was decided to raise the
vertical dimension 3-4mm by measuring the actual
values of vertical dimension at rest and vertical
dimension of occlusion of the patient. A customised
jig was made based on the vertical dimension
and patient was asked to wear it for 1 month.
Patient was recalled after 1 month. An open-tray
impression technique was selected for impression
and copings were attached (Fig.6). The prepared
acrylic custom tray was marked according to the
impression coping and the tray was adjusted for
the proper placement with impression copings
intraorally. Addition silicon was used in putty and
light- body consistency in a single step. Once the
material set impressions copings were incorporated
into impressions and screw was unscrewed and
impressions were carefully removed in the single
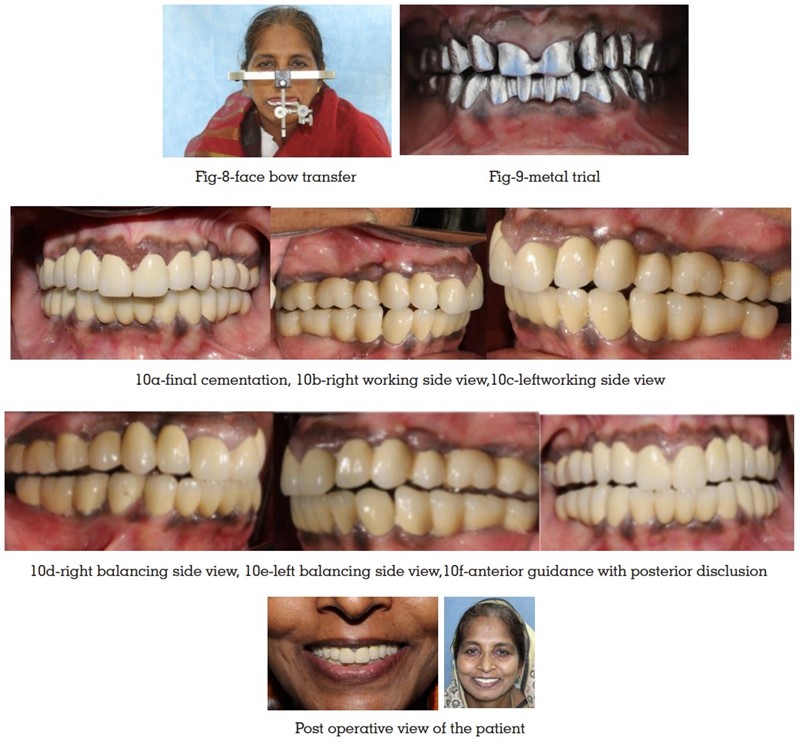
stroke to prevent the distortion. Abutment jig trial
was done. A bite registration (Fig.7) and face
bow transfer (Fig.8) were done and mounted on a
semiadjustable articulator. Metal trial was carried
out (Fig.9), followed by bisque trial and occlusal
corrections were done. The final prosthesis were
cemented with minor adjustments (Fig.10). Group
function occlusion was planned for the prosthesis.
Post-operative instructions were given to the patient
and the patient was kept under regular follow up.
Proper diagnosis and treatment planning is key to
any successful mouth rehabilitation. Implant Full-mouth rehabilitation is also designated as implant
complete mouth rehabilitation. Successful implant
treatment involves osseointegration of implants that are placed in ideal positions for the fabrication
of a dental prosthesis. Surgical placement of
dental implants is a well-documented treatment for
edentulism7
. Treatment success rates are high and
postoperative complications were relatively modest
in implant supported fixed partial denture. It not
only provides good satisfaction on patient’s behalf,
but also increased psychological confidence and
social activity than with conventional overdentures.
With all modifications in the techniques, the
primary need for the prosthesis is to produce a
passive fit for the fixed implant prosthesis and
arguably one of the most technically important
phases in implant dentistry.
Implants have become treatment of choice in
many, if not most situations when missing teeth
require replacement. Appropriate diagnosis and
treatment plan are required for a successful full
mouth rehabilitation. Careful integration and
sequencing of the different areas of treatment
need to enhance the final result.