Cyst is a pathological cavity filled with fluid, semifluid or gaseous content lined by epithelium and not created by the accumulation of pus. Cysts of the jaws are treated by enucleation and marsupialization. After the removal of the cyst, space-occupying stent is fabricated for faster healing and patient comfort. Stents are appliances constructed to cover the tissues or the teeth for their protection, to carry medicaments, radium material, to control bleeding, to determine radiographically the prospective site of dental implant. Stents are used for shaping the alveolar process or positioning of gingival tissues. It enhances faster healing of the wound by preventing food impaction. We are reporting a case of mandibular multilocular cyst that was treated by enucleation and post-surgical stent.
Key words: Post-surgical, Stent, Mandibular multilocular, Cyst.
Cysts of the jaws are treated in one of the four basic methods: Enucleation, Marsupialization, a staged combination of the two procedures, and Enucleation with curettage. Enucleation has been effective and reliable method to treat cysts. It is complete removal of cystic capsule, without rupture of its lining reducing the possibility of recurrence.1-2 Here we are presenting a clinical case report of a mandibular multilocular cyst in a male patient that was treated by enucleation followed by fabrication of stent.
A 20-year-old male patient reported to the
department of prosthodontics with a lot of pain
and discomfort after the removal of multilocular
cyst. The medical and family history was not
significant. The past dental history reveals that
patient’s chief complaint was swelling and pain in
the left mandibular region. On examination, extra-orally there was mild swelling on the left side of his
face, with normal appearing skin. (Fig:1) Further
investigation showed root stump with respect to
36. The radiographic examination revealed a
large well-defined homogeneous radiolucency
extending from tooth number 34 till 37 (Fig:2)
Surgical removal of root stumps and enucleation of
the cyst was done. Post surgically patient reported
to the Prosthodontic department with pain and
discomfort. On examination a huge hollow space in the body of mandible was seen in relation to
missing 36. (Fig: 3) The treatment plan suggested
to the patient was surgical stent. This case report
explains the steps involved in fabrication of stent.
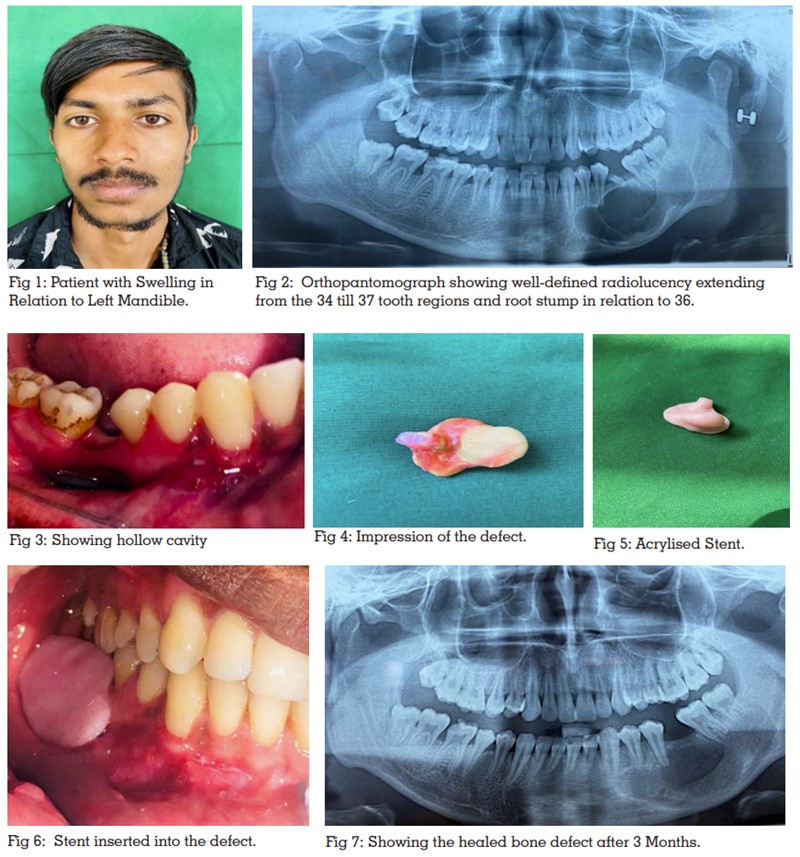
The defect was irrigated cleared of food debries. The Mandibular impression was made using irreversible hydrocolloid impression material and the cast was poured using dental stone. The custom tray was fabricated using self-cure acrylic resin extending to the hollow defect. The tray was adjusted impression of the defect was made using low fusing impression compound. Undercuts were blocked using modelling wax. (Fig:4) Impression was directly invested using dental plaster. Acrylization was carried using heat cure acrylic resin following routine protocol. The stent was deflasked trimmed and polished (fig:5). The stent was tried in patient’s mouth and necessary adjustments were made. The stent was inserted from lateral direction engaging the defect and extending onto the ridge as shown in the figure 6. The patient was recalled for regular checkup every week. Patient was feeling comfortable and the pain reduced considerably after using the stent. Figure 7 shows healing of defect in the region from 34 to 37.
Post-surgical stent enhanced the healing by preventing food lodgment into the defect, reduced halitosis, maintained better oral health. Surgical wound healing period was quite comfortable and faster with less possibility of repeating infection.