Overdenture conventionally is a partial or complete denture prosthesis constructed over existing teeth or root structure. Attachments are the linchpins of an overdenture. Based on the clinical situation there are various attachment systems that are used accordingly. It is important that the clinician knows well about the attachment system and the amount of mechanical load that the clinical situation is going to deliver on the system. This article reviews the various attachment systems available in the market and their descriptions, advantages and disadvantages.
Key words: Overdenture, attachment systems, implant supported overdenture, tooth supported overdenture, stud attachments, bar attachment, magnets, telescopic attachment
Overdenture conventionally is a partial or complete
denture prosthesis constructed over existing teeth
or root structure. The use of overdenture therapy was dated back a century back and has been still
follow prosthodontists.1
Preventive prosthodontics
has become a trend and the use of overdentures
has increased to the point where it is now feasible
alternative to most treatment plan outlines in
the construction of a prosthesis for patients with
some remaining teeth or even no teeth. Implant
supported overdentures are presently one of
the best options for replacing missing teeth due
to their added advantages as well as they are
not very expensive and are within the reach of
many patients. Attachments are the linchpins of
an overdenture. It is important that the clinician
knows the attachment system well and the amount
of mechanical load that is going to deliver on the
system. In tooth supported overdentures there
are many conventional techniques including
simple tooth modification and reduction, tooth
reduction and cast coping, endodontic therapy
with amalgam plug, endodontic therapy with cast
coping utilizing some form of attachments.1
Usually, a tooth supported overdenture procedure that incorporate the use of attachments will
commonly use anterior teeth, preferably two
canines. After endodontic therapy, the clinical
crowns are reduced to the height of the adjacent
tissues. The denture is then completed and
delivered to the patient. The teeth that are to
receive the attachments are prepared following the
necessary adjustment period. A special diamond
rotary instrument is used for this preparation.9
The mostly commonly used approach for using
abutments in overdenture therapy is using
endodontically treated teeth with cast coping
using some sort of attachment. This approach
should be reserved for patients which requires
significant improvement in retention and stability.
The abutment need low caries index, adequate
bone support, good periodontal prognosis and
meticulous oral hygiene for taking the increased
stress that the attachment brings to the tooth.
Better retention is given on the casting by various
means like lengthening the post in the root canal
or by adding pins to the casting. The attachment
needs some available interridge space for its
construction.
Even though various types of attachment systems
are available, mainly there are four types of
attachment assemblies which are commonly used
namely:
Stud attachment
Bar attachment
Magnets
Telescopic2
Wismeijer et al. (1999)5
and Epstein et al6
had
described the absolute retentive capacity of
overdenture attachments. Based on retention,
the attachments can be classified into
According to Winkler1 they can be rigid or resilient based on the type of movement. Leung and Preiskel had suggested the resiliency of the attachments in relation to stress dissipation.7 Attachments based on resiliency are classified as2 :
Stud attachments are one of the oldest attachments
used in overdentures. It has a male stud type that
is attached to the base, which is a coping over an endodontically treated tooth stump or an implant
abutment.1
They can be divided into two groups:
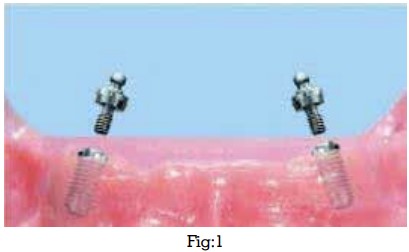
Ball attachment, Locaters, O-ring attachments,
Extracoronal Resilient Attachment (ERA)
attachments are very commonly used. ERA
attachments are rigid attachments and are
considered best for parallel implants. For clinical
application with implant-supported overdentures
ball attachments are considered as the most
simplest type of attachments. But, the main
drawback of this system is that the O-rings loose
retention with time and to be replaced periodically.11
If implants are nonparallel and angulation is >15°,
stud attachments cannot be used.2
To overcome
this disadvantage of stud attachments, locaters
were developed in 2001.12 Also stud attachments
provide two movements-vertical and hinge,
whereas locators has universal hinge movement.
The major areas to be considered while aligning
these attachments is its relation to one another
and to the path of insertion of denture.
Their advantages are that it can be used in cases
of limited inter-arch space and can accommodate
inter implant angulations up to 40°. Locator
attachments provide two types of retention, one
which is mechanical and another is frictional. The mechanical retention is given by outer margin of
attachment engaging the shallow undercut area
on abutment. Since the nylon male component
is slightly oversized than its female component it
gives a frictional fit. Locator attachments are used
without an inner retention feature so that they can
correct implant angulation.12
Disadvantages of using locator attachments are
that they cannot be used in cases where rigid
restoration is required and due to constant wear
and tear, regular replacement of male nylon part is
needed. In a retrospective no significant difference
was observed between stud and bar attachments.14
Some stud attachments can be entirely rigid
because of their small size. Springs and other
devices have been incorporated in some designs
so as to allow for some movement. Gerber, Dalbo,
Zest, ERA, Prosnap, Profix are different stud
attachments. Gerber is the largest stud unit.10
Gerber attachment allows vertical movement and
a rigid attachment that does not allow movement
of base. Retention is given by the spring clip in the
female housing engaging a groove in the male
section. It is easily replaceable.
Dalbo attachment can be rigid, resilient, and stress
broken, the resilient being the most commonly
used. They allow vertical and rotational movement
of the female component around a sphere shaped
male component.
Ceka attachments has male component affixed
to tooth with four sections capable of being
compressed and are flexible.
Zest anchor attachments derives retention from
within root and female component is cemented to
place. They have advantage of overcoming the
space problem that the attachment is within root
structure. Also the leverage on the abutment tooth is
negligible because the point of attachment is well
below the alveolar bone level and the attachment
procedure is simple without any casting. If more than one tooth is involved then parallelism may
not be necessary because of the flexibility of nylon
male component. They have disadvantages of
susceptibility to caries and fracture.
Introfix attachments is tall stud attachment
providing frictional retention. It is adjustable as
well as replaceable. Due to their height they are
subjected to torque and hence should be used
in only tooth supported overdentures. They also
require paralleling mandrel if more than one
attachment is used.
Schubiger attachment uses a permanent form of
fixation using a screw system. They also require
paralleling mandrel and are highly indicated for
teeth with diverging roots. They can be converted
and interchanged with Gerber attachments if one
or more abutment teeth is lost.
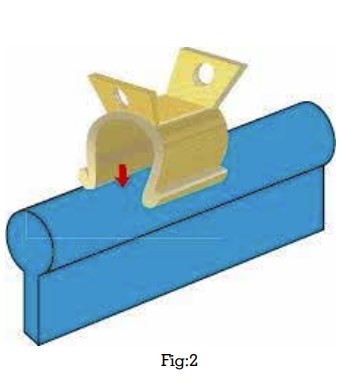
The purpose of bar attachment are splinting of
the abutment teeth, retention and support of the
prosthetic appliance. There are rigid types called
bar units and non rigid ones called bar joints.
The former is tooth borne and the later is utilizes
residual ridge support.
Hader bar system consist of preformed plastic
bars and plastic/ metal clips. Retention can be
improved by adding more clips.
Dolder bar system supplied as both bar unit and
joint. Since the bar is preformed it can approach
only close adaptation to the ridge contour because
it remains in a straight line. Retention is due to
frictional fit. They are bulkier making esthetics very
difficult. Baker clip consist of a small ‘U’ shaped
clip designed to fit over a round wire.
Ackerman and CM clip can have vertical and
horizontal movements. Due to their smaller size
and ease of fixation they are excellent option
where bar system is indicated.
Magnets were not very commonly used for dental
purposes till few decades ago. Their benefits
include simplicity, low cost,automatic reseating
after denture displacement, comparative freedom
of lateral denture movement, a low potential for
trauma to the retained roots, self-adjustment,
inherent stress breaking and no need of
adjustments.15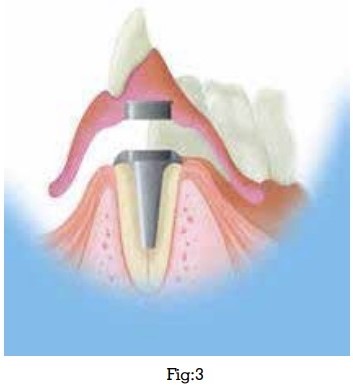
Magnets which are commonly used in implant
dentistry are basically made of aluminum-nickel-cobalt metals. As they allow all the movements of
the prosthesis, they are classified as universally
resilient attachments. But unlike the mechanical
attachments, the magnetic forces of attraction
generated to provide retention were weaker. Hence
these are not very successful to provide retention.
They can also get corroded in saliva on long-term
use.16 To overcome this, newer generation magnets
were developed which is made up of rare earth
elements such as samarium and neodymium.17
These have improved the properties of conventional
magnets.18,19
The advantages of magnetic attachments are that
as they are shorter when compared to others, they
can be used in cases of reduced inter-arch space.17
Moderately nonparallel abutments can also use
them since they do not follow a specific path of
insertion.17 Laboratory procedures associated with
castings are not necessary. They are more resilient
and hence allow easy movement of prosthesis.
Disadvantages include,attachment needs to
be removed before taking magnetic resonance
imaging because it causes streaking17, when
numbers of implants are relatively few, retention
is not as good as when ball attachments are used.
They have least retention and heating during
sterilization leads to decrease in retentive forces
in long-term use.20
The telescopic crowns have been in use since
years, to connect teeth to overdenture, but their use
in an implant supported overdenture is limited. As
they provide rigid attachment they are sometimes
used for immediate loading. But due to its design
they require adequate inter-arch space to be used,
in cases where sufficient inter-arch space is not
present it cannot be used. The new syncone system
is been used in immediate loading cases.20
The syncone system contains of prefabricated
titanium abutments and their corresponding gold
retainers with 4-6° taper. The abutments are able
to correct the angulations by 15° and can rotate
360° for better alignment. Gold retainers fit on
titanium abutments and has excellent retention
which also improves over time due to the settling
phenomena.20
Advantages of telescopic crown techniques are
that they give excellent immobilization of the
restoration, flexibility of design, easy maintenance
of oral hygiene. The syncone system has wear
resistant attachments and also be used on
angulated abutments.
It is critical that the appropriate attachment be
used for each individual patient situation. These
classification systems helps in having a broader
view about the type of attachment to be used in
each clinical situation for which an attachment
is intended.
In 1976 George L et al, in his article discusses
a method of overdenture construction using the
Dolderbarjoint attachment. He said the teeth
selected as abutments should have approximately
one-third of the supporting alveolar bone remaining
and no more than Class II hypermobility.22
Reducing the clinical crown of periodontally
involved abutment teeth brings the support for
the overdenture bar more closer to the bone. The
mobility can be reduced by cross arch splinting,
Use of Quinlivan attachment showed satisfactory
follow-up report in a case reported by Nair V et.al
in 2020, in which use of metal press button is found
to be a simple technique to fabricate overdenture
attachments economically.23 Chen T et al did a study
to evaluate patient satisfaction and masticatory
efficiency between two attachments-locators as
stud attachment and magnetic (Magfit) attachment
in single implant supported overdenture. Even
though locator attachment showed a better chewing efficiency than Magfit attachments, there
were no reliable statistical significance.24 In a finite
element analysis John J et al the stress distribution
around the implant supporting mandibular
overdenture using two attachment- ball/O-ring
and magnetic, was evaluated and concluded
that if larger diameter attachments are used then
implants with greater diameter can reduce the
stress on the cortical bone.24 The meta-analysis by
Chaware SH evaluated the various attachments
and suggests that ball attachments give excellent
outcome when the number of implants is less and
when more than two implants are possible, bar
or locator attachments give better outcome. He
also concluded that in maxillary arch splinted bar
attachments are can be used and in mandibular
arch, locators or un-splinted ball are preferred.
Among all ball and locator attachments has been
documented with excellent survival, favorable
tissue response, and good patient satisfaction
especially in case for mandibular overdentures
through various studies.
There has been various attachment system used in
tooth and implant supported overdentures. But to
provide a successful treatment, the clinician should
have a thorough knowledge of various attachments
available, their use and adaptability in various
clinical situations,benefits and demerits of using
it. While using any particular type of attachment
system clinician should try to fulfill almost all
the necessary requirements which are essential
for stable and successful esthetic and functional
rehabilitation of that system.
No financial support received for this article.
There are no conflicts of interest.