The aim of this review article is to present various ceramic materials currently utilized in the field of CAD/CAM. Due to high aesthetic and functional demands of indirect restorations research on dental materials is increasing. Comparing the materials will take into account their mechanical properties, their clinical usage, their advantages and disadvantages.
Key words: CAD/CAM; dental ceramics; biocompatibility dental materials; mechanical properties
CAD/CAM stands for computer-aided design and
computer-aided manufacturing. As a means of
accelerating the design process and easing its
transition into production, CAD/CAM is applied
across various fields of engineering, science, and
even art1. The purpose of this review is to highlight
its constantly growing role in dental prosthetics,
more specifically, in bridges, onlays, crowns and
veneers. CAD/CAM allows us to provide patients
with implants, inlays, onlays and crowns and veneers that are placed on dental implants2. It is
possible for a dentist to scan a patient’s dental
cavity, design and make their restorations, and
bond them in a matter of hours because of the
technology used in CAD/CAM.
There is no doubt that CAD/CAM technology is very
innovative and offers a wide range of opportunities.
CAD/CAM systems may not be enough to achieve
correct teeth relations in clinical cases regarding
patients with maxillomandibular disorders
and occlusion distortions . As a consequence,
restorations exceeding the height and width of the blocks cannot be designed or milled. This
reveals clinical problems including occlusal
vertical dimensions that are inaccurate and
centric relationships that are incorrect. Digital
scans are more accurate when the arch included in
the impression is short . Different types of materials
can have different survival rates when it comes
to CAD/CAM restorations. The Vita Mark II (VITA
Zahnfabrik, Bad Säckingen, Germany) ceramic
material showed a survival rate of 90.6% after 8 years and 85.7-89% after 10 years3. As a result, the
survival rate decreases with time. Among Zirconia based restoration patients with periodontal disease
or conservative reasons, lasers can be used. There
is a possibility that lasers can adversely affect
the surface of restorative material. According to
Romanyk, et al., subtractive machining causes
surface and subsurface damage to the restorations
which may have clinical relevance.
In recent years, CAD/CAM software providers
(e.g., CEREC SW 5.1.3, Dentsply Sirona, York,
PA) and manufacturing systems have emerged
in great numbers. There are two types of CAD/
CAM systems: in-office and laboratory systems
[35]4. Both of them are complex and contain many
components. Among Sirona’s offerings are the
CEREC Omnicam scanner, CAD/design and CAM
software, as well as the CEREC MC, X and XL 4-axis
milling machines. Carestream Dental (Atlanta,
GA), Dental Wings (Montréal, QC, Canada) and Zfx (Dachau, Germany) are other examples of
CAD/CAM systems used5. Several companies offer
parts included in CAD/CAM systems that can be
bought separately as well. Dental professionals
usually choose an appropriate system based on
their experience and office equipment, but patients’
therapeutic needs must also be taken into account6.
Computer-aided manufacturing uses a variety of
materials.. An example of the CAD/CAM block
before processing is shown in this figure.
Dental ceramics
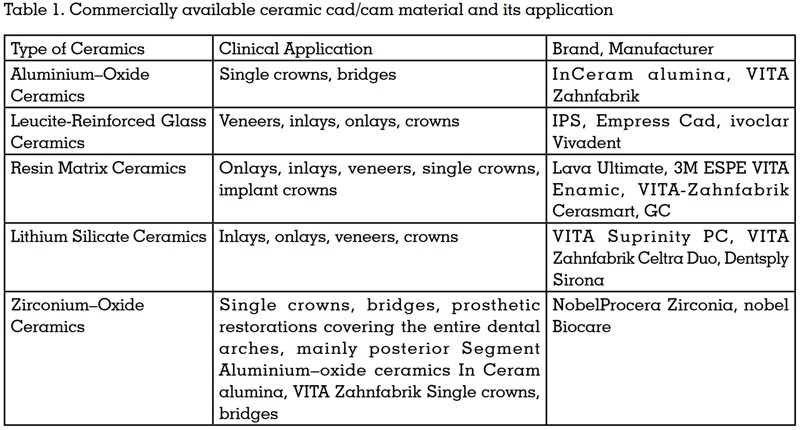
Ceramic type has a different clinical application
due to its properties (see Table 1).
Resin Matrix Ceramics
This is a relatively new material on the market, but
it is said to show some beneficial properties for
dentures. Resin-based ceramics are characterized
by good milling performance, higher load capacity
and better elastic modulus compared with silica based ceramics5. Compared with pure ceramics,
the manufacturing process of VITA Enamic ensures
a lower fracture tendency and superior CAD/CAM
processing performance. In addition, their optical
properties are similar to those of natural teeth, and
compared to ceramics, they are characterized by
lower tooth wear.
Silicate Ceramics
These are non-metallic inorganic ceramic materials
containing a glass phase. Examples of silica-based
ceramics are Vitablocs TriLuxe from Vita and
IPS Empress Cad multi from Ivoclar Vivadent.
They have good optical properties, such as high
transparency and natural appearance. Studies
evaluating the tensile bond strength of lithium
disilicate ceramics have confirmed that etching the
bonding surface of restorations with hydrofluoric
acid is still the “gold standard “.7
Leucite-Reinforced Glass Ceramics
Discussed the long-term clinical evaluation of
leucite-reinforced glass repair ceramics (such
as Duraceram and Dentsply Degussa). Leucite reinforced ceramics are not recommended for
posterior dental crowns, because compared with
other glass ceramics, leucite-reinforced ceramics
have lower mechanical properties8. However, their
aesthetic quality is sufficient and in recent years,
it has been replaced by lithium silicate ceramics,
which has better physical properties and sufficient
optical properties
Lithium Silicate Ceramics
Some sources claim that lithium silicate ceramics
(for example, Ivoclarivoclar Vivadentvivadent,
Schaan, Liechtenstein’s IPS e.max CAD, VITA
Zahnfabrik’s VITA Suprinity PC and Dentsply
Sirona’s Celtra Duo) are the strongest of all
available silicate ceramics. Its flexural strength
is about 407 MPa. First, lithium disilicate ceramics
was introduced to the market in 1998 (IPS Empress
2).9
(see Table 2)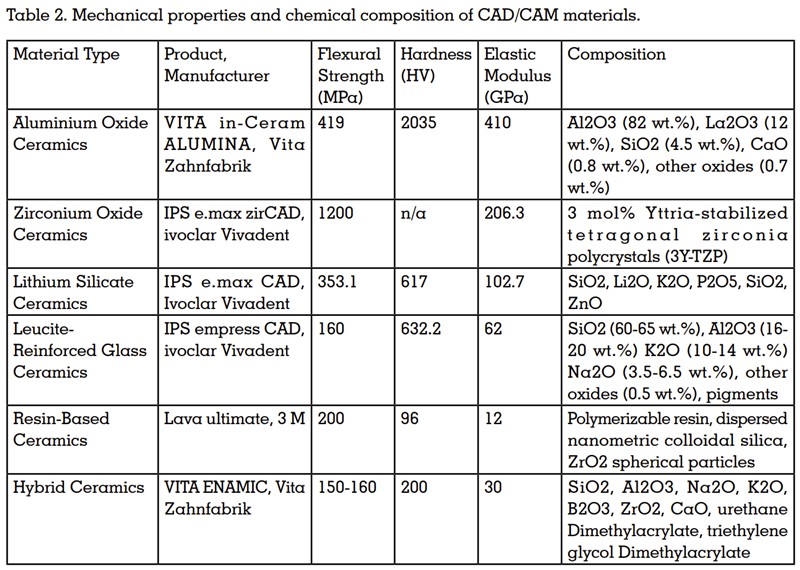
Successful and stable bonding leads to high
clinical success rates over the long run. CAD/
CAM restorations are largely recommended for
resin bonding and self-adhesive resin cements.
A. Mine et al. created a review providing a broad
outlook on the bonding procedures of CAD/CAM
materials.10 A hydrofluoric acid etching procedure
should be carried out before bonding to create
microretentive surfaces.11 Afterward, silanization is
performed in order to ensure chemical adhesion.
Study characteristics of the bonding procedure
for CAD/CAM polymer-infiltrated ceramics (such
as Vita Enamic) are compared with indirect resin composite materials (such as the Lava Ultimet,
KATANA AVENCIA block, Gradia Block, Ceras-Mart
and Block HC). There are general recommendations
for bonding CAD/CAM materials, but they may
vary depending on producer recommendations
and clinical operators’ experiences. A technical
and scientific document from Vita Enamic
provides an example of the bonding process12. The
author proposed the following scheme: use VITA
CERAMICS ETCH (5% hydrofluoric acid gel) to
etch for 60 seconds, and then use VITASIL, VITA or
Monobond Plus, Ivoclar Vivadent for silanization.
Adapting the newly placed dental restoration to the
oral cavity’s conditions is extremely important, not only regarding their shape, but with the mechanical
and physical properties as well.
Compatibility with the surrounding tissues is
crucial in the biological aspect. In the context of
cytotoxicity, biocompatibility is an interdisciplinary
concept that encompasses biological, chemical and
physical interactions and is closely related to the
concept of cytotoxicity. A CAD/CAM material must
possess the mechanical, chemical, and thermal
properties of human bone in addition to being
biocompatible with the surrounding tissues. The
material should not cause any irritation, swelling,
or intolerance in the oral cavity. Biocompatibility
must therefore be considered when evaluating
potential materials. Surface roughness and
type determine adhesion. CAD/CAM materials
used for CAD/CAM were studied for adhesion and development of microorganisms that form
biofilms13. Accordingly, IPS e.max and polished IPS
e.max showed the best ”anti-adhesion properties”
against Streptococcus mutans and Lactobacillus
rhamnosus. Additionally, Materials 2021, 14, 1592
15 of 21 concluded that the ceramic materials
(lithium disilicate) showed a superior response
to the cells.
Ceramic materials are becoming more accessible
and easier to handle in CAD/CAM. Modern ceramic
materials for CAD/CAM are described along with
their mechanical and clinical properties, which
enable long-term success of restorations. Selecting
the right material also requires clinical experience.
To produce a successful prosthetic restoration,
the technique must always be customized to each
individual patient. An occlusal plan may not be
able to be defined in the case of maxillomandibular
relationship disorders. In order to meet the
patient’s individual needs, material and method
selection must be individualized for each case.
The use of this technology provides not only a
high quality, professionalism & profit but also a
steady increase of a new and satisfied patients
and are easy to use.