Obturator prosthesis is required for the restoration of speech, deglutition, and improvement of esthetics in patient after maxillectomy. The presence of oral tumors necessitates the surgical removal of all or part of the maxilla, leaving the patient with a defect that compromises the integrity and function of the oral cavity. The maxillofacial Prosthodontist, as a member of the surgical team, plays an important role in the recovery and rehabilitation of maxillectomy patient by fabricating and placing a surgical obturator. This clinical report describes the use of definitive hollow bulb obturator with cast partial denture framework for the treatment of a 65-year-old patient with hemimaxillectomy. This technique will improve the speech, mastication, swallowing and esthetics for the patient.
Key words: Cast partial denture framework, Hemimaxiilectomy, Hollow bulb obturator
Rehabilitation of maxillofacial defects can be
challenging for maxillofacial Prosthodontist.
Frequently, the contiguity of oral cancer
necessitates the surgical removal of all or part of the maxilla, leaving the patient with a defect that
compromises the integrity and function of the oral
cavity.1,2 Postsurgical maxillary defects predispose
the patient to hypernasal speech, leakage of fluid
into the nasal cavity, and impaired masticatory
function. The prosthesis needed to repair the defect
is known as a maxillary obturator. An obturator
(Latin: obturare, to stop up) is a disc or plate, which
closes an opening or defect of the maxilla as a
result of a partial or total removal of the maxilla.3
The primary objective of intraoral prosthesis is to
enhance function i.e. swallowing, mastication and
speech thereby enhancing the psychological well
being of the individual.4
Successful obturation
depends on the volume of the defect and the
positioning of the remaining hard and soft tissues
to be used to retain, stabilize and support the
prosthesis.5
The hollow bulb obturator design is
an aid to improve the retention and the resonance
of voice as it is light in weight.6, 7 Thus hollow
obturator is the treatment of choice in such cases.
This clinical report describes the fabrication of a
hollow definitive obturator with cast partial denture
framework for a patient with a unilateral acquired
maxillary defect to improve retention, stability and
support of the obturator.
A 65 year old male patient reported to Department
of Prosthodontics, Vasantdada Patil Dental College,
with a chief complaint of difficulty in speech and
mastication. The patient’s dental history revealed
that he had undergone surgical resection of left
maxilla. He had a small soft tissue mass in oronasal
region which went on gradually increasing and
experienced breathlessness. The soft tissue mass
was removed along with adjacent tissues and
alveloar structures resulting into palatal defect.
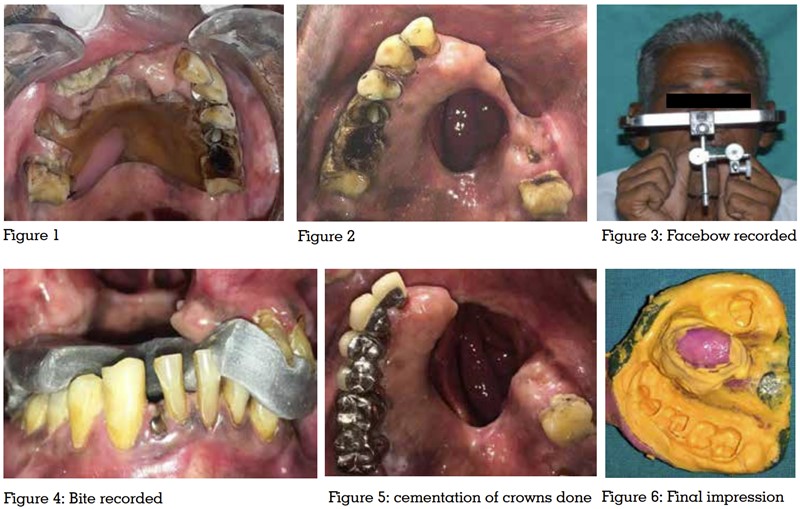
After 7-8 days the patient was given a delayed
surgical obturator which he was using since 10-11
years (figure 1). Patient was not able to explain
about detected pathology and neither report
regarding his past treatment was maintained
by the patient. On intraoral examination, class
1 Armany maxillectomy defect was found on the left side.8
The resection involved the hard palate,
alveolar bone, teeth, and soft tissue. The operated
site was well-healed. The Missing teeth were 11
and from 21 to 26 (figure 2). Severe attrition and
extrusion of lower anterior teeth with reduced
vertical dimension of occlusion.
In this present case the treatment objectives were:
The patient’s surgical obturator was relined and used as interim obturator without bulb.
Establishing lost vertical dimension by giving
crowns on remaining maxillary teeth followed
by definitive hollow bulb obturator with cast
partial denture framework replacing missing
teeth were planned. Initially, an alteration in
surgery from prosthetic point of view, the mucosal
band connected to palatal defect was resected 3
months back to favorable type of defect to facilitate
retention, stability and support. The maxillary and
mandibular diagnostic impressions were made
with irreversible hydrocolloid. Cast was poured
with dental stone. Face bow record was made
using orbitale as anterior point of reference and
maxillary cast was mounted on Hanau wide Vue
articular using facebow transfer. Mandibular cast
was mounted using centric relation record.
The bite was raised by 3mm, as there was loss of
vertical dimension and the mockup was done.9
Tooth preparation for metal ceramic restoration
was done with minimal occlusal reduction. The
retraction was done. Impressions of the prepared
teeth were made with vinyl polysiloxane. New
facebow record was made (figure 3). A centric
record was made with bite registration material
(figure 4).Temporization was done. Wax patterns
were fabricated with cast partial framework components. The crowns were examined with
Cingulum rest seat on 13, Occlusal rest seat
on 14, 16 distally and mesially on 15, 17 and
27 and finally luted with glass ionomer cement
(figure 5). Then undercut areas were blocked on
diagnostic cast and spacer was adapted over
cast. Auto polymerizing resin custom tray was
fabricated for making final impression. Border
moulding was done in defect area using low
fusing compound (DPI Pinnacle Tracing Sticks).
The final impression for definitive obturator was
recorded using light-body elastomers (3M ESPE
Soft putty) (figure 6). The master cast was made
in die stone (Kalabhai ,Ultrastone) & duplicated
in refractory material. Cast partial framework was
planned with components. Embrasure clasp in
relation to 14, 15 and 16, 17; Cingulum rest on 13;
occlusal rest on 27; modified complete palatal type
major connector extended till palatal surfaces of
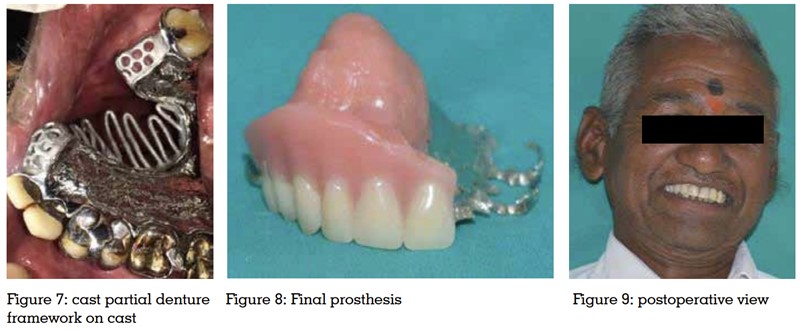
teeth.10 Partial framework of the cast was fabricated
with the help of various wax patterns. Casting
of the metal framework was carried out. Trial
of the finished and polished framework on cast
& intraorally (figure 7) was done and needed
adjustments were done. Wax occlusal rim was
made on the framework. The jaw relations were
recorded. After teeth arrangement try-in was done.
The final prosthesis was fabricated with heat cured resin material (figure 8). Final prosthesis was
adjusted in patient’s mouth (figure 9). Occlusal
adjustments were done to make passive contacts
on defect side. Final prosthesis was functionally
and esthetically pleasing.
In this present study, the patient had a well healed defect so rehabilitation has been achieved
with definitive hollow bulb obturator with cast
partial denture framework. Hollow bulb provides
advantages such as reduction in weight and
making prosthesis comfortable. Here, Cast partial
framework was planned for prosthesis because;
with well-extended hollow bulb obturator it offered
adequate retention, satisfactory occlusion, stability,
durability and increases longevity.
Declaration of patient consent
The authors certify that they have obtained all
appropriate patient consent forms. In the form the
patient(s) has/have given his/her/their consent
for his/her/their images and other clinical
information to be reported in the journal. The
patients understand that their names and initials
will not be published and due efforts will be made
to conceal their identity, but anonymity cannot be
guaranteed.
Financial support and sponsorship
Nil.
Conflict of interest
There is no conflict of interest.