Prosthodontic rehabilitation with complete denture in compromised edentulous ridges through standard, customary techniques is a difficult task. Treatment procedures require remodeling as per the patient’s desire for esthetics and functionality. This article presents a case series of various techniques used for administering compromised ridges. These techniques have been found helpful in enhancing stability of denture and masticating ability by changing the pattern of teeth arrangement.
Key words: Compromised ridge, lingualized occlusion, neutral zone, piezography technique.
The crucial determinant for a successful denture
therapy involves carrying out of the treatment plan
with utmost precision, based on comprehensive
history and through oral inspection. This kind of
a treatment plan should be based on Devan’s1
rehabilitation principles that is, preserving
what already exists and not just replacing what
is missing. Ridge atrophy poses many clinical
challenges in the fabrication of an effective prosthesis. Residual ridge resorption is a complex
process and a common occurrence following
extraction of teeth. It is most striking during the
initial period of tooth loss, subsequently leading to
slower but continuous rate of resorption.2
Factors
influencing rate of resorption are divided into
anatomic, metabolic, functional, and prosthetic
factors.3
Anatomic factors comprise of the shape,
size, and density of ridges as also the thickness
and the distinctive features of the mucosa. Cellular
activity of osteoblasts and osteoclasts is influenced
by metabolic factors which include nutritional
status and hormonal balance. Frequency, duration,
severity and direction of forces are other functional
factors which are responsible for cellular activity.
Prosthetic factors consist of various methods,
materials, concepts and principles, that are
practiced during prosthetic procedures.
According to the concept presented by Fish and
Mathew the neutral zone is stated to be that part in
the mouth where the outward forces of the tongue
are negated by the cheeks and lips forces pressing
inwards. (GPT-9)4
. When the alveolar ridge is lost
to a great extent, the steadfastness and the firm
hold of the denture rely upon the proper position
of the teeth and outline of the external surfaces
of the dentures. Forces acting upon the buccal surfaces of the teeth and the polished surfaces of
the denture are in horizontal position. When the
teeth are not in contact, the direction and extent
of forces and the position of impression surface
defines the stability of denture.5
The lip influences
the lower denture stability and is essential as the
ridge resorption becomes more or as the patient
grows old. As the alveolar ridge resorbs, it has
been seen that the ridge crest falls below the origin
of the mentalis muscle. As a result the neutral zone
is positioned posteriorly and it becomes necessary
to position the lower anterior teeth further lingually
as compared to original position of the natural
teeth.6
The forces of displacement act on the lower denture
through tongue, the lower lip and the modiolus. If
the denture is positioned in the region in such a
manner that it balances these displacing forces,
then the denture will become more stable when in
function. If the denture stays outside the neutral
zone it will be not remain firm and secure while
talking, swallowing and masticating.7
The neutral
zone technique has many advantages which are
(1) increased strength and grasp (2) the rear
teeth will be placed in correct position to provide
enough tongue space; (3)minimized food trapping
close to the molar teeth; and (4) enhanced face
appeal because of facial support. Piezography
and lingualized occlusion are other techniques
which help in providing stable denture base in
compromised ridges.8
Klein9,10 in 1974 introduced a method, named
piezography, which recorded the prosthodontic
space for teeth placement using speech. It is used
for fabrication of complete denture in a patient
with long-standing edentulism and severely
resorbed mandibular ridge. The theory behind
placement of artificial teeth in the neutral zone
has two aims: Firstly, the teeth will not restrict the
normal functioning of the muscle and secondly,
the forces exerted by the musculature against the
dentures will be make it more stable and will have
more retention. Piezography helps to record the neutral zone. speech is employed for recording
the denture space.11,12,13
Payne & Pound first suggested the basic concepts
of lingualized occlusion[14] It is an endeavor
to safeguard the esthetic and food-penetration
benefits of the anatomic form while retaining the
mechanical independence of the non anatomic
form. For maxillary denture the lingualized concept
uses anatomic teeth and nonanatomic teeth for the
mandibular denture.14 In case of severe resorption,
narrow occlusal table is preferred.14 Various case
reports are discussed below based on different
techniques for better stability of mandibular
denture with resorbed ridge.
A male patient aged 54 visited Manav Rachna
Dental College, Faridabad, Haryana. He had been
suffering from edentulism for the last 6-7 years.
On intraoral examination it was found that his
maxillary ridge was in favourable condition, but the
mandibular ridge was not in a good functional state
due to excessive resorption. According to Atwood
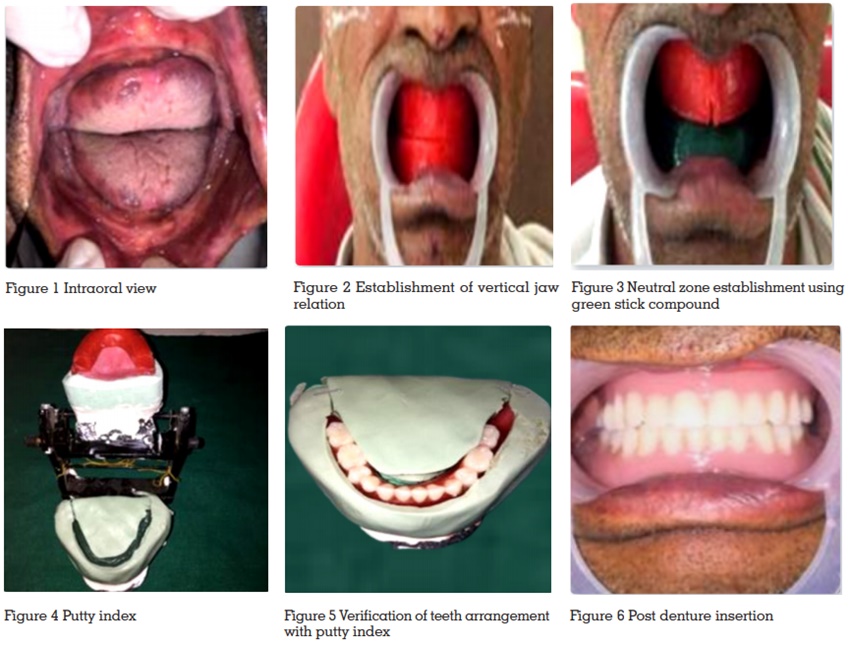
classification it fall under Order-4.(Figure-1) Then
it was decided to fabricate lower complete denture
by Neutral zone impression technique.
Procedure
Diagnostic impression is made with impression
compound (DPI) followed by border moulding
with green stick compound (DPI) and final
impressions with zinc oxide eugenol paste (DPI).
Later record bases were fabricated, and their
stability was evaluated. Wax rim is contoured on
the upper denture base conventionally. Fox plane
is essentially used for orientation of the maxillary
rim, followed by the establishment of the occlusal
plane. Later midline, distal of canines, and smile
line was marked on the maxillary rim. Tentative
jaw relation is done followed by articulation (Fig 2).
Soften the green stick compound uniformly and
place it on the lower record base. Then the record base is inserted in the patient’s mouth and the
patient is then asked to suck and swallow so that
the green impression compound (DPI) is moulded
into the neutral zone area8,9 (Figure 3). Record base
is removed and inspected. Record base is then
placed in the articulator and an index is made for
fabrication of new wax occlusal rim according to
the index (Figure 4). Teeth arrangement is done
on the articulator and verified with the index
(Figure-5), later it is tried in patients mouth. Denture
is fabricated in conventional way (Figure-6)
A male patient aged 62 years, visited the
Prosthodontic department of Manav Rachna Dental college, mainly complaining of edentulism
and inability to chew. On oral examination it was
seen that the patient had a severely resorbed
mandibular ridge, loss of vertical dimension,
collapse of facial profile and loss of muscle tonicity.
Lack of nutrition was also evident due to inability
to chew food properly. Due to severe resorption,
conventional method was not considered and was
decided to implement piezographic technique to
manage the case.
Procedure
Primary impressions were made using admixed
technique in which impression compound (DPI,
Pinnacle) and green tracing stick compound (DPI) were used in 3:7 parts by weight then primary cast
were obtained. Custom trays were fabricated and
final impressions were made using zinc oxide
eugenol impression paste (DPI) for both the
maxillary and mandibular ridges.
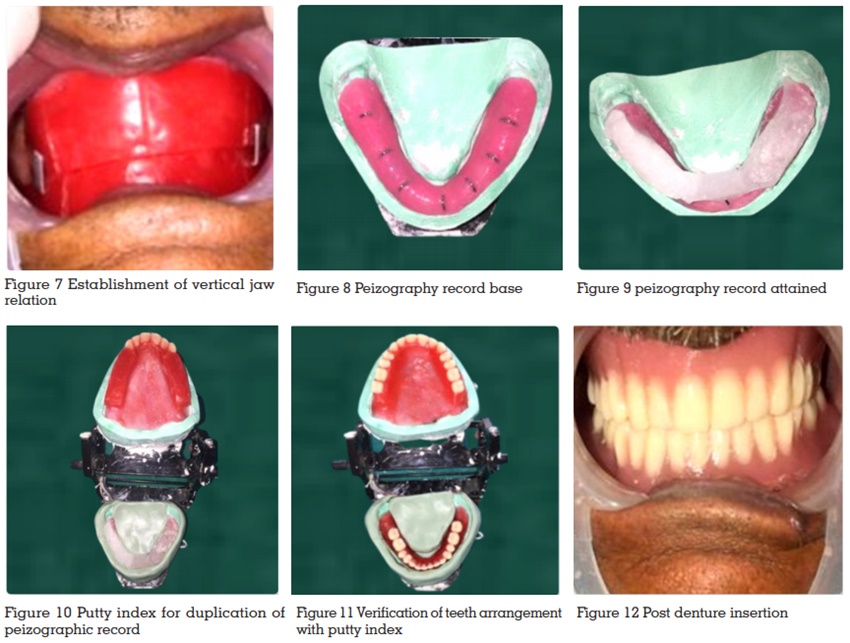
Occlusal rims were fabricated. The upper rim was
adjusted parallel to the Camper’s line and 2 mm
visibility was established. The vertical dimension
both at occlusion and at rest was recorded. A
freeway space of 2 mm was maintained (Figure 7).
On a mean value articulator wax rim along with
cast assembly was mounted. The piezographic
method was carried out from this position onwards.
Since the technique was based on phonetics, the
patient was made to practice pronouncing certain phonemes before actually implementing it. The
speech exercise helped mold the material that was
inserted in the mouth providing the prosthodontic
space.
Another record base was fabricated from self-cure
acrylic resin (DPI). Grooves were made on the
external surface and vertical v shaped slots were
made with orthodontic wire so that the moldable
material can adhere to the acrylic and those slots
provide retention to the material11 (Figure 8).
A silicon-based self-polymerizing temporary
soft liner was used (Dentsply visco-gel). Prior to
placement of the base plate in the mouth, silicon
adhesive was generously applied on top of the base plate for better adhesion.
The maxillary rim was placed in the mouth.
Upper anterior teeth were arranged as they help
in improved speech during the pronunciation of
phonemes
Initially, the soft liner was first placed on either
right or the left side and the patient was instructed
to pronounce the phonemes. Once the material
set, the piezographic record was checked and the
same was done for the contra lateral side
The patient was asked to say ‘SIS’ four times
followed by a strong ‘TO’ in order to obtain the
posterior molding.11 After the posterior dam was
obtained, moldable material was placed anteriorly.
Anterior piezography was obtained by asking
the patient to pronounce T, D, M, P five times in a
sequence clearly and vigorously.11
Excess was removed with a knife and adjusted to
the required height (Figure 9). Later this record
base is put on articulator and putty index was
made so as to obtain new rim for teeth arrangement
The wax rim was adjusted to the predetermined
vertical dimension and placed in the articulator.
The posterior teeth were now arranged in the newly
obtained space (Figure 11).
The waxed up teeth arrangement was tried intra
orally to evaluate esthetics and speech. Dentures
were fabricated conventionally and inserted.
Occlusion was satisfactory. Facial profile improved
drastically and the denture was stable functionally.
A male patient aged 59 came to the department,
primarily complaining about inefficiency to chew
properly and he wanted a new denture. Based on
oral examination, it seemed that lower alveolar
ridge was in resorbed condition. Conventional
method was not considered and we decided to
implement lingualized occlusion technique to
manage the case
Procedure
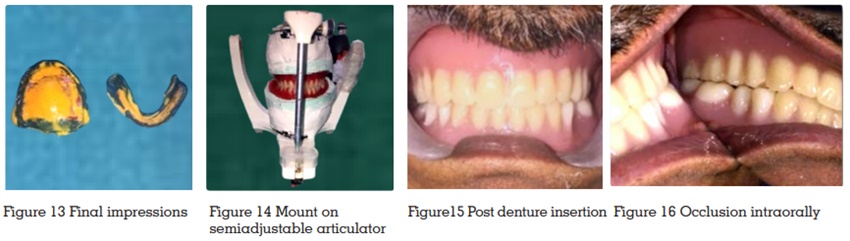
Impression compound (DPI, Pinnacle) was used
to make preliminary impression. Custom trays
were then prepared on primary cast. After border
moulding was completed then final impressions
were made in (Zhermack Zetaplus) light
body impression material (Figure13). Maxillo-mandibular relation was recorded using the
conventional method based on Camper’s plane.
Mounting on semi adjustable articulator was done
(Figure 14).
Artificial teeth were arranged in lingualized
occlusion comprising maxillary anatomic teeth
while mandibular non anatomic posteriors. In
this only maxillary palatal cusps should contact
with mandibular central fossa in centric occlusion,
maxillary buccal cusp should not touch15,16,17.
This arrangement allows the food bolus to get
excellent penetration. Bilateral equilibrium is
maintained mainly by the maxillary lingual cusp
which establishes contact during excursions with the inclines and central fossae of the mandibular
cusps17. Maxillary anatomic teeth preserves
aesthetics and maintains chewing capacity while
mandibular non anatomic teeth reduces horizontal
forces. Moreover Vertical forces are directed more
centrally on the mandibular alveolar ridge, which
gives more stability to the lower denture.17 Later
dentures were fabricated by the conventional
method.
The one difficulty faced while fabricating the
severely resorbed mandibular denture is stability.
This problem can be taken care of when dentures
are constructed with outlines harmonizing with
neutral zone. Neutral zone technique aims at
creating a denture in muscle balance.18 It is not
necessary to place the teeth on the crest of ridge as
it is majorly dictated by the action of the muscles
and differs from patient to patient. Tooth position
and flange contour will establish how stable a
denture is. The stability of the polished denture
surface depends upon the action of buccinators,
orbicularis oris and the contraction of the muscles
of tongue, cheeks and lips.18 The shape of this
complicated surface, more than the outline of the
denture, decides whether the movements of the
muscles will displace or stabilize the dentures. The
buccinators and tongue muscles exert retentive
force on the well designed dentures, resulting
in better control of the patient on the dentures
even in resorbed condition.19,20 The buccinator
muscle and the tongue give the bracing effect to
the flanges of the lower denture when extended
underneath. The mandibular denture should be
narrow in the premolar area, that is the region
of modiolus, to prevent the denture from being
raised while in function, and the posterior teeth
must not infringe on the tongue posteriorly.20
The neutral zone is dictated by width, form and
intraoral position which varies from one person
to another. Also the neutral zone is impacted by
numerous techniques, material, muscle tone and period of edentulism. Therefore in atrophic ridges
it is greatly recommended to record neutral zone
in fabrication of complete denture.
A successful prosthodontic treatment of a
patient with a poor mandibular alveolar ridge,
is dependent on many factors. It is important for
a prosthodontist to understand the constraints of
the patient, the prosthodontic treatment methods
available, the limitations of the oral surgeon, and
the capabilities of the laboratory technician. The
prosthodontist may decide upon a more traditional
or customary methods of treatment or may use
more advanced prosthodontic techniques using
sophisticated instrumentation or the oral surgeon’s
discretion to perform extensive and augmentive
procedures upon the patient. The severely
resorbed mandibular ridge can be restored to a
level of masticatory function although the task is
challenging.