The gradual wear of the occlusal surfaces of teeth
is a continuous phenomenon. Excessive occlusal
wear may lead to occlusal disharmony, pulpal
trauma, esthetic disfigurement, and impaired
function. Management of tooth wear is challenging
in preventive and restorative dentistry. Correct
assessment of occlusal vertical dimension,
interocclusal rest space, and centric relation records
are critical for successful treatment. Innovations
and well-defined specializations have widened the
treatment realm for tooth preservation as well as
tooth replacement. The treatment of these patients
is complex, There are vital guidelines that can
help to achieve a successful outcome.
Anterior guidance is crucial in human occlusion
because it influences molar disocclusion that
controls horizontal forces. Molar disocclusion is
determined by a cusp-shape factor and an angle of
hinge rotation1
. The three factors which determine
disocclusion are: condylar path, incisal path and
cusp angle. Hobo and Takayama stated that, “the
condylar path shown to have deviation within
the individual and its influence on disocclusion
is minimal”.2
This article presents prosthodontic rehabilitation
of a patient with multiple missing teeth, severely
worn dentition and uneven occlusal plane has
been treated using twin stage procedure.
A 71 year old male reported to the Department of Prosthodontics, Mahe Institute of Dental Sciences, Mahe with a chief complaint of multiple missing teeth and severe wear of dentition since few years which is getting deteriorated over a period of time. Patient was hypertensive and on regular medication since 10yrs (Cilacar 10mg)
Extraoral examination shows facial asymmetry
with more muscle development on left side of face.
Well developed (Class 1) Masseter. Brachycephalic
head and Euryprosopic face. No abnormality in
the TMJ.
Intraoral hard tissue examination shows Mild
calculus and stains. Generalised attrition. Bony exostoses and cervical abfractions. Alveolar bone
buttressing Teeth missing :36,37,47 Fractured
amalgam restoration on 35
Supra-eruption of 17,18,27,28. Tenderness on
percussion :14, Secondary caries :14 Edge to edge
bite. Soft tissue examination shows Generalized
periodontal pockets with average probing depth
of 4mm. Mild gingival enlargement in relation to
upper & lower anteriors (drug induced). Evaluation
of edentulous ridge : Siebert’s classification Class
II. Generalised gingival recession.

Excessive wear without loss of vertical dimension of occlusion but with space available (Turner and Missirlain Category 2) The case was taken for the following objectives of treatment to:
A heat cure clear acrylic occlusal splint of 3 mm
was given to the patient for 6 weeks. The adaptation
of the patient to the increased VDO was evaluated
during 2-month trial period. Muscle tenderness and
temporomandibular discomfort were not found.
Extraction of 14,17,18,28,38 and Root canal
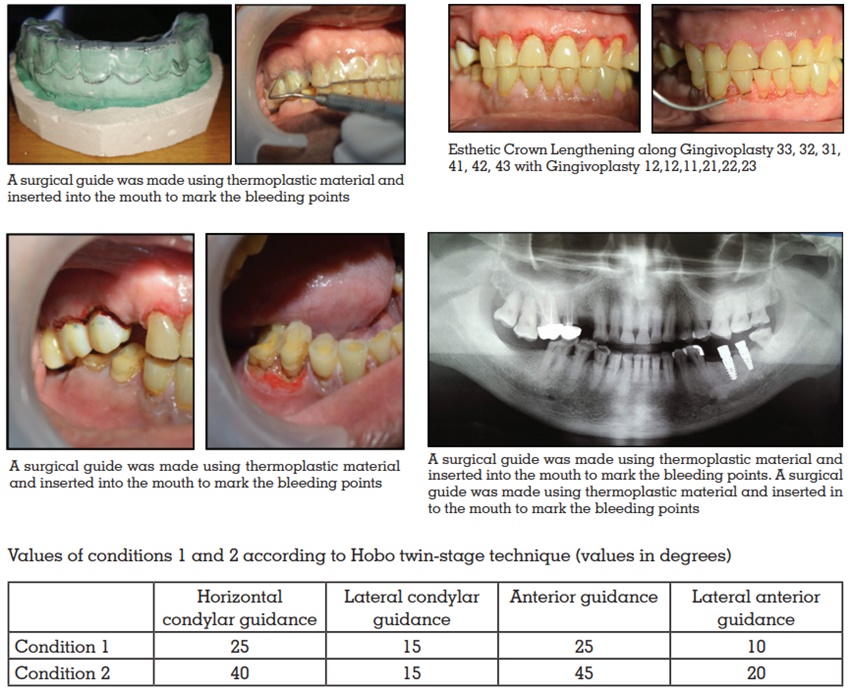
treatment of of 13,12,24,25 26,36,35,34,33,32,42,43 was performed. Functional crown lengthening of
15,16,45,46. Aesthetic crown lengthening along
with gingivoplasty in relation to 13,12,11,21,22,23.
Gingivoplasty in relation to 33,32,31,41,42,43.
Implant was placed in relation to 36 and 37 Size
4.2×10 & 3.75×10 (Adin System).
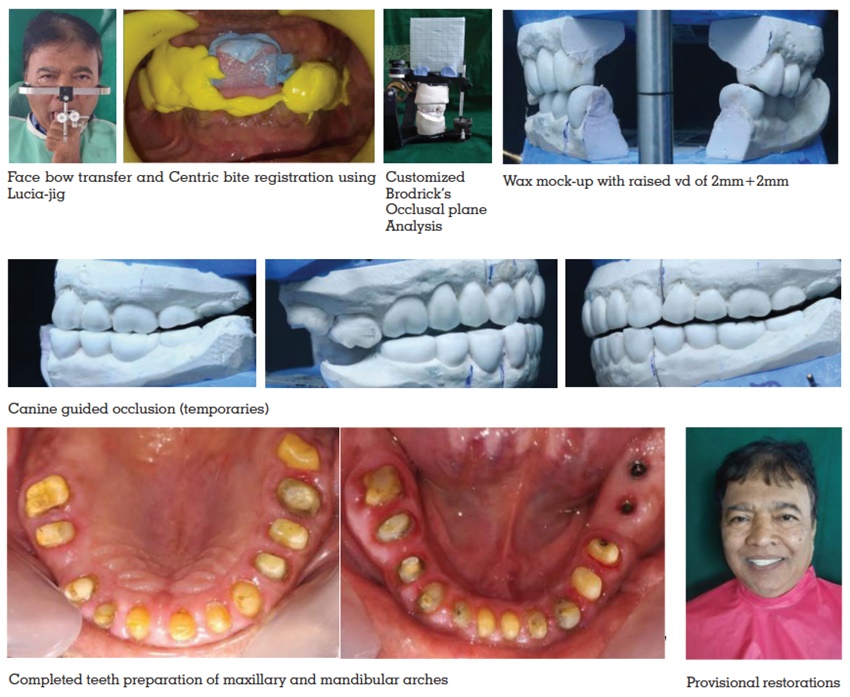
The diagnostic impressions were made using
irreversible hydrocolloid. The patient’s casts were
mounted on a semiadjustable articulator (Hanau
H2) using a facebow record at increased VD.
Mandibular occlusal plane was analysed using the Broadrick’s occlusal plane analyzer. Divider
of Broadrick occlusal plane analyzer was opened
at 4 inches and a mark was obtained on the flag
by keeping one end at the distal end of the canine
and the second end of the divider at the distobuccal
cusp of the last molar and another mark crossing
the first one was obtained. Now, another end of the
divider was kept on this intersection of the marks,
and occlusal plane was marked on mandibular
canine.3
Occlusal equilibration was done in
the patient’s mouth by removing the occlusal
interferences, so that centric relation coincided
with the maximum intercuspal position.
The semiadjustable Hanau articulator was
programmed to Condition 1 of Hobo’s twin-stage
procedure wherein after removal of the maxillary
anterior segment, posterior segment diagnostic
wax-up was done in bilaterally balanced occlusion.
The settings were changed to Condition 2 where the
maxillary anterior segment was replaced and the
anterior wax-up was completed and checked for
proper anterior guidance to achieve disocclusion
in eccentric movements due to canine-guided
occlusion. Provisional crowns were fabricated with
autopolymerizing resin using a vacuum‑formed matrix produced from the diagnostic wax-up.
The interim restorations were kept for 45 days to
assess the patient’s adaptation to the proposed
new occlusal scheme and vertical dimension of
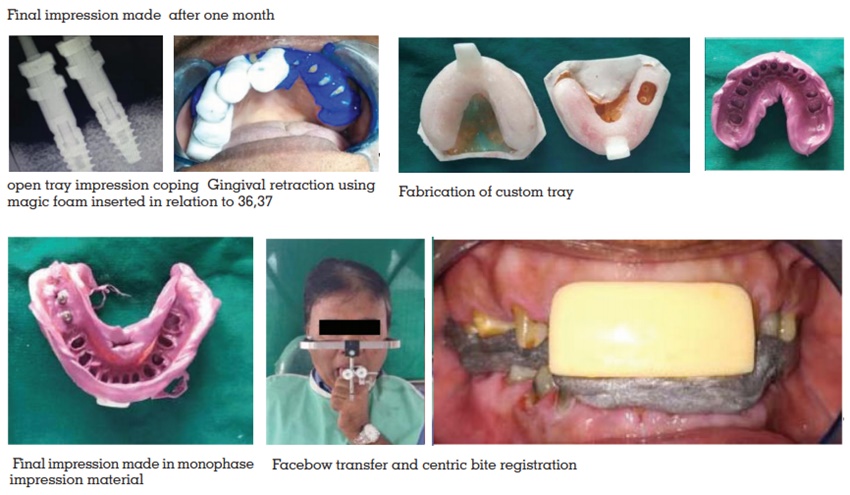
occlusion, which was raised by 3 mm. Once the
patient was satisfied with temporary restorations,
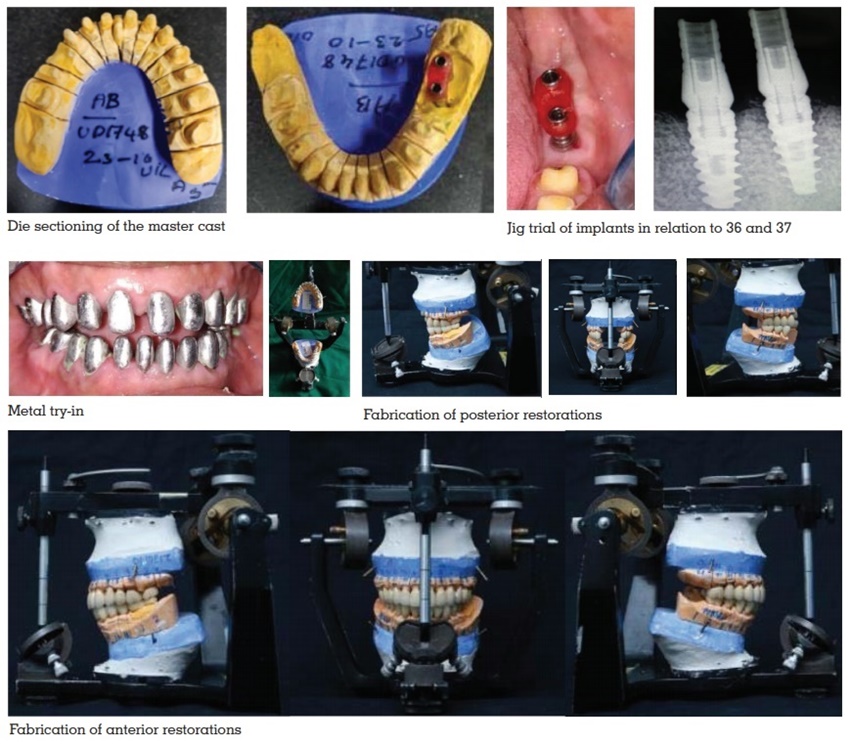
the definitive cast was fabricated. After die cutting,
the casts were
mounted on semiadjustable articulator. The wax
patterns were fabricated, invested, and casted.
The metal copings were retrieved and metal try-in was done after finishing. After the metal try‑in,
the ceramic was applied and bisque try-in was
completed. Porcelain-fused-to-metal restorations
were made using Condition 1 and 2 of Hobo’s
technique. The canine-guided occlusion was
checked in the mouth, and after verification,
the crowns were cemented with temporary
polycarboxylate cement. After 2 weeks, once the
patient was comfortable, all the crowns were
cemented with resin‑modified glass ionomer
cement (FujiCEM; GC America, Alsip, USA).
Postoperative orthopantogram was taken, and
oral hygiene instructions and regular checkup were
administered. The final prostheses were fabricated
on the definitive cast by using the same values that
were used to fabricate temporary prosthesis. The
porcelain fused to metal restoration was corrected
for occlusal prematurity in the mouth and it was
finally cemented. On frequent recalls, patient gave
satisfactory reviews with the treatment which was
provided.

Rehabilitation of patients with compromised
dentition is a challenge in terms of establishing
function and aesthetics for the patient4
. Thorough
examination diagnosis, and choice of appropriate
occlusal scheme are the key to successful
prosthodontic rehabilitation.5
All our efforts for
full-mouth rehabilitation are directed toward
reestablishing a state of functional efficiency, in
which the hard and soft tissues of the stomognathic
system function in synchronous harmony6
. Dawson
stated that interocclusal space is never lost and
any loss is compensated by tooth eruption, alveolar
bone expansion, and muscle action. Success in
maintaining severe wear cases depends on the
development of proper incisal guidance to allow
for proper disocclusion within patient’s envelop
of motion6,7.
The etiology of tooth wear is multifactorial,
and clinical controlled trials of restorative and
prosthodontics approaches are limited in quantity
and quality.6
The VD should be raised with occlusal splints before starting the treatment, and
the overlay prostheses should be tried between
3 weeks and 5 months for deprogramming of
temporomandibular joint.8
The severe wear of anterior teeth facilitates the loss
of anterior guidance, which protects the posterior
teeth from wear during excursive movements.
Collapse of posterior dentition results in loss of
normal occlusal plane and decreased vertical
dimension8
The incorporation of posterior disocclusion avoids
harmful lateral forces as suggested by Hobo.
In the twin stage procedure, as cusp angle was
the main determinant of occlusion; the need
to record condylar path was not necessary.6
Therefore, complicated instruments, such as the
pantograph and fully adjustable articulators are
not required. This procedure is much simpler than
the standard gnathological procedure, yet it follows
gnathological principles12.
As was stated by D Amico, cuspid protected
occlusions and disocclusions were natural
adaptations which were used for preventing
destructive occlusions13. Stuart and Stallard in
1957 said that the cuspid protected occlusion
concept had many advantages over the group
function. Hobo and Takayama said that amount of
disocclusion depends on the condylar path, incisal
path, and the cusp angle.2
Posterior disocclusion is
very important in controlling harmful lateral forces.
This case has demonstrated that if the condyles
are seated in centric relation, additional restorative
required space may be obtained. Proper anterior
guidance not only is essential for preventing the
interferences in the condylar envelop of movement
but also prevents the excessive wear.6
Hobo and Takayama studied the influence of condylar path, incisal path, and the cusp angle
on the amount of disocclusion and concluded that
cusp angle was the most reliable determinant
of occlusion.2
The twin-stage procedure helps in
achieving a standard disocclusion of 1.1 mm on
protrusion, 1 mm on nonworking side, and 0.5 mm
on working side in eccentric movements at 3-mm
protrusion from centric relation.6
However, if the
sagittal condylar path of the patient is steeper
than the articulator adjustment values (40°),
disocclusion increases. If the path is less than
40°, then the amount of disocclusion decreases.2
If the patient has less than 16° sagittal condylar
inclination (only about an 8% occurrence rate),
cuspal interferences will occur. If the incisal path
is more than 5° steeper than the condylar path,
patients complain of discomfort.8,9 Abnormal curve
of Spee and Wilson, abnormally rotated teeth,
and inclined teeth are contraindications of this
technique14
The choice of restoration in this case was porcelain
fused to metal as this would double the mechanical
durability, recover esthetics, and protect the
residual dentin.15,16
Proper diagnosis and multidisciplinary treatment planning with adequate knowledge and judgement are paramount for success. This technique relies on the factor of cuspal angle and it uses the standard values which are proposed in the twin stage technique, to achieve a centric occlusion and an excursive disocclusion.