Single complete dentures pose a great challenge to clinician. Chances of denture fracture are more when natural teeth are present in opposing arch. Heat cure acrylic resin cannot resist the heavy occlusal loads alone and it leads to denture fracture. This problem can be solved by use of innovative materials and appropriate techniques. Metal mesh reinforcement in denture provides satisfactory and economic solution for such cases. This case report describes a procedure of fabrication of metal mesh reinforced single maxillary denture, which is easy to fabricate and better in resisting masticatory loads of natural mandibular teeth.
Key words: Single denture, Metal mesh, Denture fracture.
The conventional acrylic resin denture fracture
is a challenging condition to prosthodontists.
Most common fractures are midline denture
fractures as reported in a recent dental survey.
Midline denture fractures 46.87% were seen in
maxillary complete dentures and 61% were seen
in mandibular dentures.1
The incidence of midline fractures increases in case of single maxillary
dentures opposing natural mandibular teeth.2
There are several factors contributing for denture
fracture including flexural fatigue resulting from
cyclic deformation and factors which alter the stress
distribution of the base.3,4 To avoid such fractures,
advancement in materials and techniques is prime
requirement. Use of metal reinforced denture
base,5
acrylic resin base reinforced with wire
netting, carbon fibre, E glass fibre reinforced
PMMA,6,7 lucitone 199, Trevalon high, Paladon
ultra and visible light polymerized resin8
are
different methods of increasing denture fracture
resistance and decreasing chances of failure. Out
of all these methods, metal mesh reinforcement
is an economic and less time-consuming method,
which significantly increases the denture strength.9
This case report describes a case of single
maxillary denture fabrication reinforced by use
of commercially available preformed metal mesh.
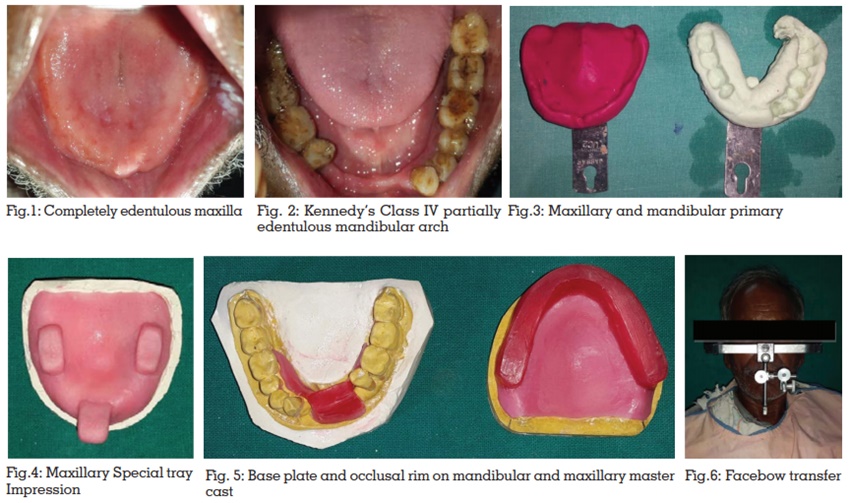
A 57-year-old male patient reported to Department of Prosthodontics and Crown & Bridge, with the chief complaint of difficulty in chewing due to missing upper and lower teeth. Patient had no significant medical history. Intraoral examination revealed completely edentulous maxillary arch (Fig.1) and kennedy’s class IV partially edentulous mandibular arch (Fig.2). Patient was explained about different treatment options-
Due to financial reasons, Patient was not willing to
go for implants and cast metal maxillary denture.
Metal mesh reinforced maxillary denture with
mandibular removable partial denture was
selected by patient. It was an economic option
with the benefit of increasing strength and fracture
resistance of denture.
Denture fracture results from two different types of
forces, namely impact and flexural fatigue. Impact
fracture occurs due to sudden blow to the denture
or accidental dropping of denture from hands or
mouth. Flexural fatigue occurs due to repeated
stress of lower dimension constantly, which
results in micro cracks formation in denture base.
Conventional denture base material Poly methyl
methacrylate (PMMA) shows poor mechanical
properties when put in an environment of heavy
occlusal loading and tends to fracture.10 Repeated
denture fracture is a problem for both patient and
clinician.11
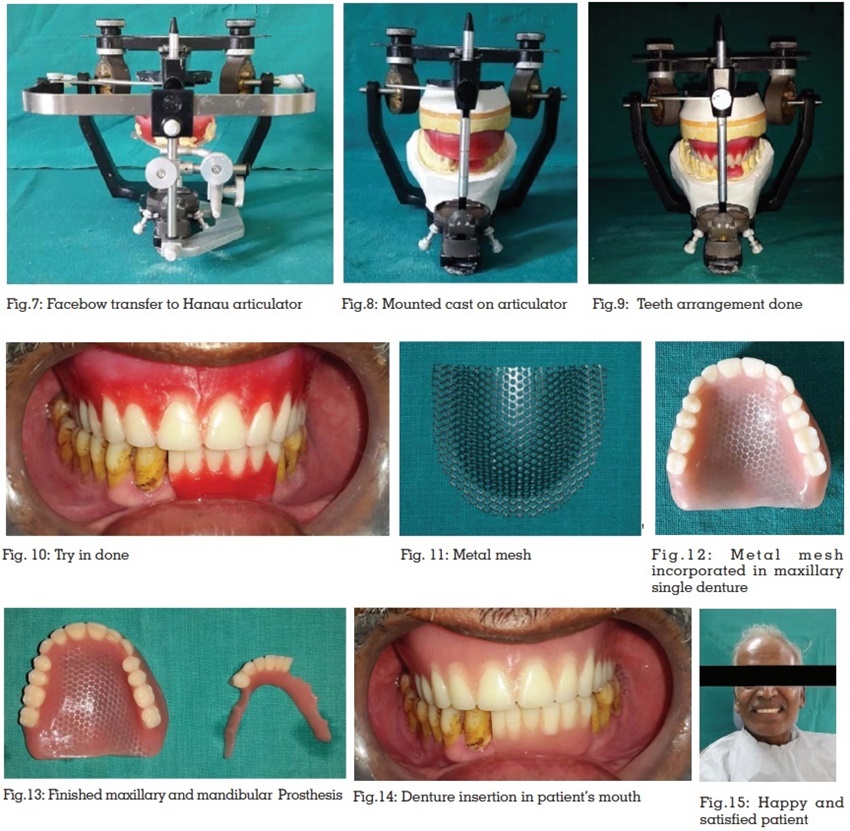
Metal strengthener has a beneficial effect
on the fracture resistance of the polymethyl
methacrylate.12 Metal base and metal mesh
reinforcement increases the strength of denture
and reduces the micro crack propagation. Metal
mesh is commercially available in both stainless steel and gold plated metal. They have a thickness
of 0.4mm and their mesh design helps to produce
a good resin bond. Metal mesh does not increase
the denture weight and decreases the chances of
fracture.13,14 Metal mesh is also economic to patient.
Stock perforated trays, which are used for making
alginate impression can be cut and modified to
be inserted in denture. Modified portion of tray is
used for reinforcing the denture.15
Using metal mesh has few disadvantages. It
looks unaesthetic if it appears on labial portion of
denture when patient smiles. It is prone to corrosion
and has poor adhesion to acrylic denture base.
In some cases patient may be allergic to metal
contact. Some authors have proposed a technique
of masking colour of metal mesh using self cure
acrylic resin to avoid unaesthetic display of metal.16
Advancement in materials and techniques is
required to completely fulfill the requirements
of patient and clinician. Implant supported
overdentures are newer treatment approach for
single dentures.17 Due to financial reasons, not
all patients can afford implant treatment. Metal
mesh reinforcement is an economic and promising
solution for such cases.
It is a challenge for prosthodontists to provide
successful treatment for patients presenting one
completely edentulous arch opposing natural
teeth in other arch. Such condition places more
amount of force on single denture. Metal mesh
reinforced dentures offer better strength and
fracture resistance. This is a viable treatment
option for all patients who suffer from repeated
denture fractures due to heavy occlusal loading.