Social and psychological well being of a patient directly or indirectly depends upon their facial beauty. Any of the maxillofacial defects will alter the quality of life, blemish the social integration and collapses the patient’s expectation to return to normalcy. Orbital exenteration is enforced to treat various neoplasms or non-malignant diseases. Conventional or implant retained orbital prostheses may be indicated, to recreate the appearance of the patient. For patients who cannot afford implant retained prostheses, orbital prostheses fabricated from silicone, and retained by mechanical means such as spectacles, or adhesives,present an economically viable treatment option. This case report presents a simplified method of fabricating the silicone orbital prosthesis in a patient with a history of orbital exenteration due to carcinoma of sebaceous gland.
Key words: Orbital exenteration, orbital prosthesis, silicone elastomers
Patients requiring treatment with orbital prosthesis are those who have lost orbital structures through exenteration. Orbital exenteration is performed by an ophthalmic surgeon for the treatment of potentially life-threatening malignancies or implacably progressive conditions unresponsive to other treatments.1 Indications for orbital exenteration include neoplasms like basal cell carcinoma, squamous cell carcinoma;painful blind eye; infection; recent injury; disfiguring blind eye; prevention of sympathetic ophthalmia etc.2 This will scourge the cosmetic, functional and psychological problems in the patients.
Patient usually dissent the cosmetic rehabilitation with reconstructive surgical procedures because of the need for further surgical procedures, added cost, and multiple postoperative visits. In such cases, the patient must be motivated for the prosthetic rehabilitation in time.3
This case report presents a simplified method of fabricating the silicone orbital prosthesis in a patient who was referred to the Department of Prosthodontics from MVR Cancer Institute, Kozhikode, for cosmetic rehabilitation after orbital exenteration due to carcinoma of sebaceous gland. The method described here was found to be cost effective, easy to perform, and resulted in the restoration of facial esthetics and overall wellbeing of the patient.
A 67 year old male patient was referred from the MVR Cancer Institute, Kozhikode, for cosmetic rehabilitation after orbital exenteration. History revealed exenteration of the left eye, following carcinoma of the sebaceous gland 1 year ago as seen in Figure 1. Clinical evaluation revealed complete healing. A tissue undercut was observed on the superolateral aspect of the left eye which was thought to provide retention for the prosthesis. Due to economic constraints, implant retained prosthesis was ruled out by the patient, while he consented for silicone orbital prosthesis retained by mechanical undercuts and tissue adhesives.
A modified impression tray was prepared using modelling wax as seen in Figure 2, to record an impression of the defect, peripheral tissues, and normal side. Patient was placed in supine position on a dental chair, and petroleum jelly was applied on eye brows and eye lashes for ease of removal of the impression. A direct impression, was made with irreversible hydrocolloid material. The impression material was poured gradually and gently until it covered more than half of the modified impression tray, gauze pieces were placed before its setting and plaster was added. The gauze piece provided strength and mechanical retention between alginate and plaster. Fast setting plaster was spread over entire surface to provide strength as seen in Figure 3.
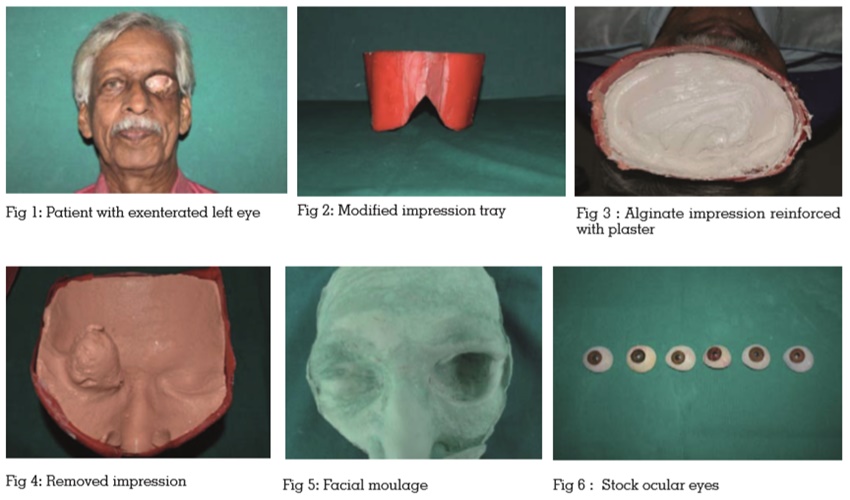
After setting of plaster, impression was removed gently and inspected for voids as seen in Figure 4. Impression was disinfected using Cidex (2% gluteraldehyde) after which it was poured in dental stone to obtain facial moulage as seen in Figure 5.
Wax pattern of orbital prosthesis was fabricated on working cast, and a prefabricated eye conformer (stockocular prosthesis) was selected as per size and color of the contralateral eye as seen in Figure 6. Wax pattern trial was done as seen in Figure 7. The position of eye shell was verified in anteroposterior, mediolateral, and superioinferior planes in accordance with the contralateral eye. After wax trial and confirmation of appropriate contour,wax pattern was returned to working cast, and sealed before investing.. Flasking was done, and after setting of plaster, deflasking was done carefully.
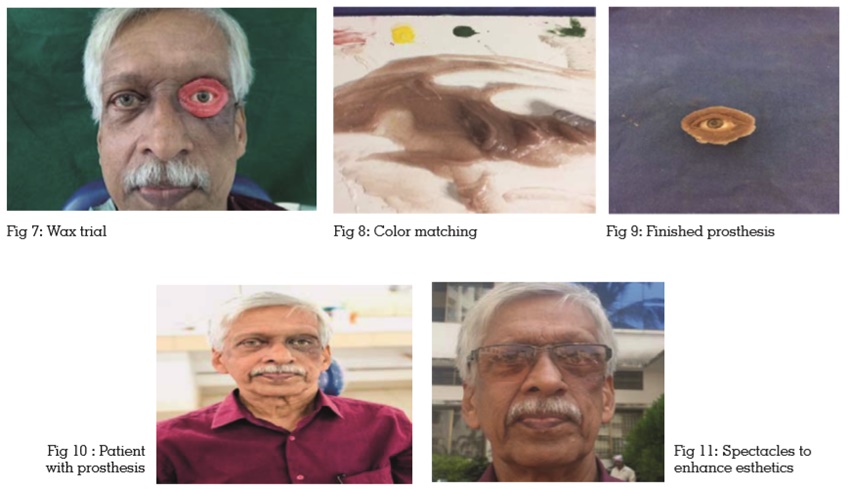
Color matching was done with skin color adjacent to defect area as seen in Figure 8.. Room temperature vulcanizing (RTV) silicone material was mixed as per the manufacturer instructions. Intrinsic stains were mixed to achieve shade matching. Packing of silicone was done, and the prosthesis was deflasked following polymerization, and finishing was done as seen in Figure 9. Artificial eyelashes were used for the upper eyelid.
The prosthesis was delivered to the patient as seen in Figure 10. Retention in the prosthesis was primarily obtained through mechanical undercuts of defect, and skin adhesives. Patient was advised to continue the use of spectacles, which could be utilized to conceal the margins of prosthesis and enhance esthetics as seen in Figure 11.
Instructions were provided regarding prosthesis insertion, removal, maintenance, and hygiene. Followup was carried out, and patient satisfaction was noted during periodic recall visits.
The main intention behind fabricating an orbital prosthesis is to ameliorate the physical and emotional status of the patient thus assuring social acceptance. Appropriate selection of the material for prostheses and the mode of retention will help the maxillofacial prosthodontist to successfully rehabilitate such patients based upon their esthetic and functional requirements. Retention of an orbital prosthesis depends on the presence of tissue undercuts, use of skin adhesives, and placement of implants.4 Implant placement was ruled out in this case due to financial constraints, hence, retention would be obtained through undercut and adhesives only. Spectacles were used to ensconce the margins of the prosthesis. Silicone elastomers are widely used to fabricate extraoral maxillofacial prostheses due to their lifelike appearance and marginal acclimatization. Nevertheless, color instability is a serious incommodity of silicones, and prosthesis may be remade every 2 years.5