Abstract: Fabrication of a successful prosthesis in hemimandibulectomy patients is a challenging task. Segmental resection of mandible results in deviation of the remaining segment of the mandible towards the resected side resulting in facial disfigurement, difficulty in speech, swallowing, respiration, mastication and certain mandibular movements are effected. Such condition develops a disturbed psychological state, affecting the daily life of the patient. The primary goal of the treatment was to achieve; facial aesthetics, phonetics and restore the function. A well fabricated prosthesis along with good patient co-operation can help to tackle such scenario more effortlessly.
Key words: Hemimandibulectomy, Non- Odontogenic tumour, Provisional removable prosthesis, Mandibular cast partial denture, Rehabilitation.
Maxillofacial prosthodontics is the world of art
and science which is full of challenges. One has
to strive hard for getting the natural function and
lifelike appearance of the prosthesis since every human has the divine right to look human. The
unilateral loss of mandibular continuity due to
surgery results in mandibular deviation toward
the defective side. The earlier the mandibular
guidance therapy is initiated in the course of
treatment, the more successful is the patient’s
definitive occlusal relationship. Obtaining proper
inter-cuspation is the key in achieving good
occlusion. Segmental resection of the mandible
results in psychological, physiological, aesthetic
problems. Prosthodontic treatment along with
certain exercise program helps in reducing
mandibular deviation and improving masticatory
efficiency. This case report describes prosthodontic
management of a hemi-mandibulectomy patient,
rehabilitated by a provisional removable prosthesis
followed by a definitive mandibular cast partial
denture designed to fulfill the patient’s needs and
requirements.
A 23-years-old male patient reported to the
Department of Maxillofacial Prosthodontics, Al-
Badar Dental College & Hospital, Gulbarga, with
a chief complaint of difficulty in chewing, facial
asymmetry, deviation of the jaw and wants to get
the teeth replaced. Past medical history revealed that the patient was diagnosed with Cemento-
Ossifying Fibroma (Commonly seen in mandible,
with 70-90% of all cases. Clinically, these tumors
manifest as a slow-growing intrabony mass that
is normally well delimited and asymptomatic –
though over time the lesion may become large
enough to cause facial deformation), for which the
patient had undergone extensive resection. After
surgical resection of the tumor,reconstruction was
done with fibular graft and fixed with recon plate.
On extra-oral examination, patient had a straight
profile, facial asymmetry, significant deviation of
mandible to the left side. Intraoral examination revealed left mandibular defect, missing teeth
from 43-41, 31-38, generalised stains and cervical
caries 44.
Based on the clinical findings and present scenario,
treatment plan was decided to provide the patient
with guide flange prosthesis to aid in correction of
the mandibular deviation, a provisional prosthesis
followed by a definitive mandibular cast partial
denture. The patient was advised for exercise
as suggested by Beumer et al. & motivated for improving the oral hygiene status at every level
of treatment.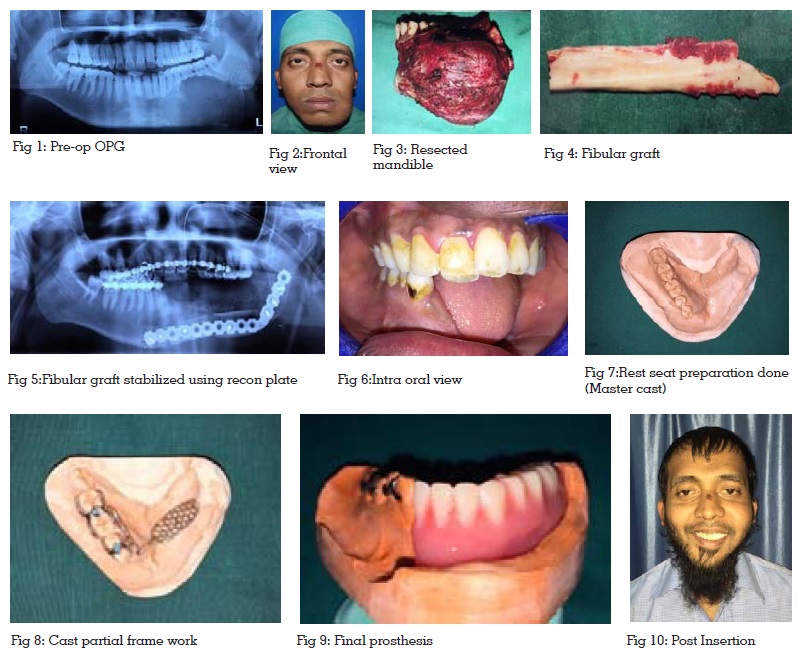
A preliminary impression was made for the
upper and lower arches and a guide flange
was fabricated using clear acrylic. Significant
improvement was noticed in patient’s occlusion
after few months. After the correction, a provisional
removable partial denture was fabricated so as
to habituate the patient for a period of few weeks.
Impression was made for upper and lower arches
using alginate impression material with stock
trays. Primary cast was obtained onto which a
denture base and wax rim was fabricated for
recording maxillo-mandibular relationship and
simultaneously shade selection was done. Teeth
were arranged accordingly in occlusion with
the maxillary teeth and try in was carried out.
The provisional removable partial denture was
then processed and acrylisation was completed.
Patient’s phonetics was improved significantly,
but retention & stability was not fulfilled by
the provisional prosthesis. Therefore definite
mandibular cast partial denture prosthesis was
further carried out.
The primary cast was surveyed and embrasure
clasps were planned on 44-45 & 46-47. Occlusal
rest seat preparation was done on the mesial
aspect of 45,47 and on the distal aspect of 44,46.
A custom impression tray was fabricated on the
primary cast so as to make a secondary impression.
The main objective of secondary impression was
to obtain retention, support and stability in the
final prosthesis. Perforations were made using
a round bur in the fabricated custom tray and
final impression was made using Putty wash
impression technique with Type I (Heavy bodied
consistency) and Type III (Light Body) Polyvinyl
siloxane impression materials. The impression
was beaded and boxed (Plaster and pumice
boxing) and poured in Type IV dental stone. The
master cast was obtained and duplicated to make the refractory cast. Surveying was done and the
metal framework was designed. Casting was
carried out and a metal cast partial framework
was checked in the patient’s mouth. Appropriate
buccal and labial fullness was checked during the
jaw relation and teeth arrangement was done. After
acrylisation, completed mandibular cast partial
denture was inserted, minor occlusal corrections
were made and post insertion instructions were
given. A remarkable improvement in aesthetics,
phonetics and masticatory efficiency was observed.
The patient was encouraged and motivated for
improving the oral hygiene and regular follow
up visits.
The need for early consultation with the
maxillofacial prosthodontist has been emphasized
in rehabilitation of mandibulectomy patients.
Mandible is a single bone that creates peripheral
boundaries for the floor of the oral cavity.
Muscles of mastication are bilaterally attached
to the mandible to generate a variety of complex
mandibular moments useful in speech, swallowing,
mastication etc. Loss of mandibular continuity
results in deviation of remaining mandibular
segment toward the resected side primarily
because of the loss of tissue involved in the surgical
resection. Greater the loss of tissue, greater will be
the deviation of the mandible to the resected side,
thus compromising the prognosis of the treatment.
The success in rehabilitating a patient with
hemimandibulectomy depends upon the nature and
extent of the surgical defect, treatment plan, type
of prosthesis, and patient co‑operation. This article
highlights rehabilitation of hemimandibulectomy
patient who has undergone resection. Literature
review advocates fabrication of guide flange
or palatal ramp prosthesis for such patients to
prevent deviation of the mandible and to improve
masticatory function and aesthetics. Disruption of the mandible has the potential to disrupt any of the
mandibular functions; therefore form and function
are the prime consideration while rehabilitating
any mandibulectomy cases. The prognosis of the
prosthesis in such defects depends primarily on
the remaining structures available after surgery
and how well a prosthodontist can make use of
it to the best along with patient’s co-operation.