Impression making is considered to be an important step in the fabrication of any fixed or removable prosthesis. However certain pathologic conditions such as Oral submucous fibrosis associated with reduced mouth opening critically hamper the impression making procedure. Proper orientation of impression tray in such patients becomes extremely difficult due to reduced resiliency of tissues and obliteration of vestibular spaces. The problems encountered in fabrication of complete denture for these patients especially during impression making are overcome by the use of sectional trays. This article focuses on use of sectional trays during preliminary and final impression making procedure for an edentulous patient with oral submucous fibrosis.
Restricted mouth opening impose a great challenge
to the dentist in performing any intraoral procedure.
This is commonly associated with conditions like
orofacial cancer surgeries, scleroderma, traumatic
injuries, temporomandibular joint disorders, oral
submucous fibrosis etc… Oral submucous fibrosis
is one of most common pathology associated with reduced mouth opening. Oral submucous
fibrosis (OSMF) is defined as a chronic disease
of the oral mucosa characterized by inflammation
and progressive fibrosis of the lamina propria
and deeper connective tissue layers. A number
of factors trigger the disease process by causing
juxta epithelial inflammatory reaction in the
oral mucosa. Suggested contributory factors
include areca nut chewing, ingestion of chillies,
nutritional deficiencies, genetic and immunologic
processes and other factors. OSMF is a potential
premalignant condition with an incidence of oral
cancer in 3-7.6% cases.1 The presenting symptoms
of OSMF are burning pain, progressive inability to
open the mouth with difficulty in mastication and
swallowing. It is most common between 20 and 40
years of age with a female:male ratio of 3:11. This
condition is prevalent among geriatric patients with
partial or complete edentulism. Restoring function
becomes a challenge to the prosthodontist due to
patient’s clinical presentation.
Several methods have been described for use
when a standard impression tray becomes difficult
to be inserted or removed from the mouth. During
impression making, modification of standard
impression procedure is required to accomplish the fundamental step in fabrication of successful
denture. Use of sectional trays can overcome the
problem of reduced access to the oral cavity during
impression making.
This clinical report describes the use of sectional
trays for preliminary and final impression for the
patient with reduced mouth opening due to Oral
submucous fibrosis.
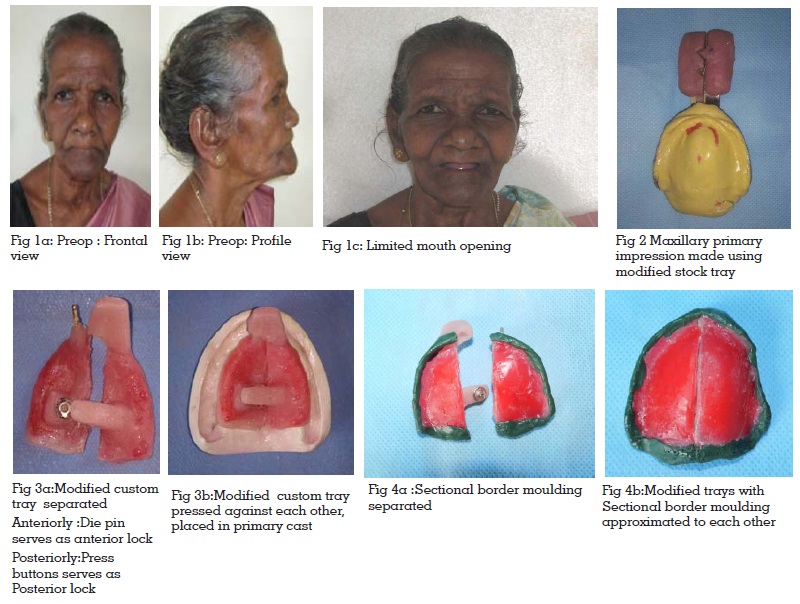
A 65 year old female patient (fig: 1a & 1b)
treated with intralesional therapy for chronic oral
submucous fibrosis reported to the Department of
Prosthodontics with a chief complaint of difficulty in
chewing due to loss of teeth. Intraoral examination
revealed the presence of palpable fibrotic muscle
bands on right and left buccal mucosa and
restricted mouth opening. The diameter and
circumference of her mouth were measured, and
found to be 30mm (fig: 1c).
Prognosis and probable prosthetic treatment
options were explained to the patient and informed
consents were obtained.
Maxillary primary impression using custom
fabricated sectional trays.
Difficulties faced in Prosthetic rehabilitation of
microstomia patients begin from the preliminary impression due to minimal mouth opening and
tongue rigidity. Hence the maximum mouth
opening does not accommodate even the smallest
of the impression trays2. Insertion and removal
of impression trays are often very difficult. To
overcome this problem, various modification in
tray fabrication have evolved which includes the
use of sectional trays2 and flexible trays3 that could
be assembled extraorally.
Impression Making
For making maxillary primary impression modified
stock metal tray was fabricated according to the
technique illustrated by K. Ashwini Kumar et al4
In this method, a stock metal tray was selected
by measuring the width of residual ridge using
caliper. The area to be sectioned was marked
on the tissue side of the tray. Later,Dental stone
was poured into the impression tray and cast was
made. This cast acted as a guide for the sectioned
stock tray. The tray was sectioned into two along
the line previously marked using a diamond disk
and the magnets were attached to the sectioned
handles with a designed reorientation mechanism.
Impression was made in two steps. The impression
of one half of the arch was made first followed by
impression of the other half. Monophase medium
viscosity impression material (Elite impression
material, Zhermack Italy) was used.
At first, the tray adhesive was applied on the both
sections of the tray and allowed to dry for 5 min.
Then the first segment of the modified impression
tray was loaded with elastomeric impression
material (Elite impression material, Zhermack,
Italy) and the impression of the corresponding
side of the arch was made. The excess material
extending medially beyond the tray was cut off,
followed which petroleum jelly was applied onto the
cut surface. Next, the second segment of the tray
was verified for proper orientation and impression
of the second half was made without disturbing
the first half. At this point, magnet incorporated, helped in holding the two segments of the tray.
The impression was taken out in segments and
was reoriented outside the mouth (fig: 2).
The impression was poured in dental plaster and
a preliminary cast was obtained.
For mandibular impression, a stock metal tray was
used according to the width of ridge.
Choosing an appropriate tray which was inserted
without any difficulty, allowed us to use a single
stock tray without sectioning and impression
was made using impression compound in a
conventional manner.
Maxillary Final impression using custom fabricated sectional trays using press
buttons:
A 2mm thick wax spacer (Maarc Modelling wax, New
Delhi) was adapted onto the maxillary primary
cast and sectioned vertically along the midline into
two halves. Maxillary custom impression tray was
fabricated using autopolymerising acrylic resin
(DPI-RR Cold cure clear) in two steps.
For the first segment,wax spacer was placed on
the cast and autopolymerizing acrylic resin was
adapted over it. A tapered brass die pin of 8mm
long was placed at an angle of 45º anteriorly in
the region of incisive papilla. This die pin served
as tray handle for this half of tray and also as a
component of anterior locking. Posteriorly, female part of press buttons were placed over the palatal
shelf 1cm away from midline that served as a
component of posterior lock.
After complete polymerization of first segment,
petroleum jelly was applied over the die pins and
also into the set acrylic to prevent fusion of two
segments. The second half of wax spacer was
adapted and acrylic resin was adapted over it to
form the second segment.
Anteriorly, acrylic resin was directly adapted
around the die pin forming a tray handle in the
second segment. Posteriorly, the acrylic plate
was extended medially over the first segment,
consisting of male part of press button forming
the posterior lock (fig: 3a & 3b).
The tray was checked intraorally, extensions were evaluated. Sectional border moulding was
completed using low fusing green stick compound
(DPI)(fig: 4a & 4b). Impression of first half of tray
was made and the excess material was cut off to
flush with second half tray. The cut surface was
lubricated using petroleum jelly and impression
of second half tray was made. At this point the
tray should be squeezed at the handle and
once precise fit was ensured, snap fit buttons
were pressed firmly and allowed the material to
set. Later, snap fit buttons were unpressed and
removed separately (fig: 5a). Outside the mouth,
trays were reassembled (Fig :5b) following which
conventional prosthodontic protocol of boxing
and pouring with type III gypsum material was
followed to create a definitive cast.
A Light body polyvinylsiloxane (Elite, Zhermack,
Italy) impression material was used. A step by step procedure for making definitive impression was
carried out based on novel technique suggested
by Suryakant.C.Deogade3.
For Mandibular final impression, sectioning of
tray was not required as the whole of custom
tray was inserted without difficulty. Hence, the
conventional procedure for final impression
making was followed(fig: 6) and definitive cast
was obtained
The handle of the tray was fabricated using acrylic
resin blocks and commercially available press
buttons were used as locks which have a male
and female part. The handle with the press buttons
function as anterior and posterior locks.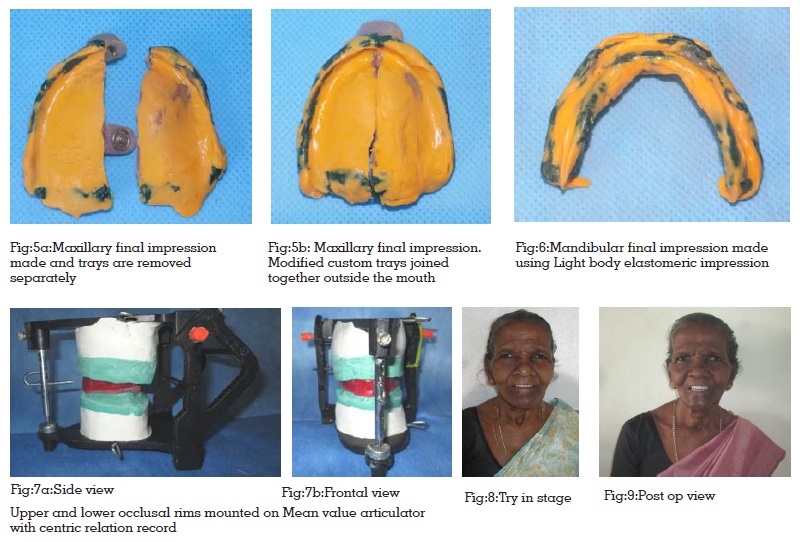
Jaw relation, Try in & Prosthesis delivery
With the obtained master cast, a permanent base
was fabricated. At this point, it was possible to place
the denture as a single piece,which eliminated the
need for construction of a sectional denture which
though would be convenient for placement would
be difficult in hygiene maintenance.
Maxillomandibular relationship was recorded
and mounted on an articulator (fig:7a & 7b).
Teeth arrangement was done;and the setup was
tried in patient’s mouth (fig: 8). The maxillary
and mandibular complete dentures were then
acrylized conventionally in heat polymerizing
acrylic resin (DPI)(fig:9).
Rehabilitation with conventional complete denture
for microstomia patients is a challenging task due
to decreased perimeter of the oral cavity. Presence
of fibrotic buccal mucosa makes manipulation of
muscles for border moulding extremely difficult. To
overcome these problems, several modifications
in tray fabrication have been illustrated in the
literature. Use of flexible trays and sectional trays
provide a helping hand in impression procedures.
Whitsitt and Battle5 described a technique for
making flexible impression trays for a microstomia patient. He had utilized silicone putty material
(Optosil, Unitek Corp., Monrovia, Calif.) that can
be inserted and molded in the mouth before it
sets. Due to its flexible nature, the silicone tray
can be easily inserted and removed. Various
authors have suggested different techniques for
fabrication of sectional trays. A variety of pins,
bolts and Lego pieces have been used for the
locking mechanism of sectional impression trays
fabricated for patients with limited oral openings6,7
Sectional impression trays have been fabricated
using recesses, orthodontic screws, Lego blocks
(Lego Systems Inc., Enfield, CT), dowel plug holes
with a screw joint for rigid connection, locking
levers, interlocking tray segments and flexible
impression trays with silicone putty.
K. Ashwini Kumar et al4 described a technique of
making sectional trays for maxillary impressions
in which magnets were attached to the sectioned
handles with a designed reorientation mechanism.
Vamsi Krishna CH et al8 described simple and
economic methods of fabrication of two-piece
custom sectional trays for patients with oral sub
mucous fibrosis.
A sectional stock tray system for making preliminary
impression was described by Luebke9. Impressions
using sectional trays may be easier for patients
with restricted oral openings because the two
halves can be inserted independently, removed
separately and reassembled extra-orally. Improved
fit of the tray was possible because the two halves
were separately fitted to each side of the arch
to achieve better anatomical adaptation to the
soft-tissues. The important requirement while
fabricating a sectional tray is the mechanism
employed to accurately adapt and stabilize the two
segments of the tray to each other both intra-orally
and extra-orally. The technique should allow easier
manipulation to decrease patient trauma. Use of
both anterior and posterior locks is important for
better stability. The technique for sectional tray
described in this report employs the use of lock
pins and press button which fulfills all the criteria.
A maximal opening smaller than the size of a
complete denture can make prosthetic treatment
challenging.
Modifications in procedural techniques help to
overcome the technical difficulties faced during
prosthetic management of patients with oral
submucous fibrosis. The technique employed for
tray fabrication is a combination of two different
lock mechanisms, which facilitated the operator
to obtain accurate impressions for patients
with restricted mouth opening. These sectional
tray designs are easier to fabricate, less time
consuming and requires relatively inexpensive
locking mechanisms.