Abstract: Complete maxillary or mandibular edentulism is considered to be the most challenging clinical condition to rehabilitate. A possible solution to provide stability and retention of the prosthesis in this condition,in a short time i.e on the day of implant surgery,is intraoral welding technique. This goal can be achieved by welding titanium bars on implant abutments directly inside the oral cavity, which decreases the risk of micromovements of implants with regard to surrounding bone and possibility of error or distortion due to prosthetic procedures.
The increase in life expectancy continuously
has brought new challenges to the dentistry, as
number of edentulous patients are increasing
in one or both arches.1 These patients often do
not accept a rehabilitation with a removable
prosthesis, for either functional or psychologic
reasons. The evolution of implant dentistry brought
an increasing interest in immediate esthetic
replacement of missing teeth. Placement of dental
implants followed by immediate loading with a
fixed, implant-supported prosthesis mimics the
biomechanics of teeth within the alveolar bone.
Biologic benefits for these patients are internal
loading on the alveolus and preventing continued resorption of the jaw bone.2
More advanced protocols decrease the healing
period, and in the case of immediate loading for
a full-arch replacement, implants are exposed
immediately to occlusal and muscular forces.
The resultant changes in both the surgical and
prosthetic protocols are remarkable and are a
significant departure from the original two-stage
protocol.2 A time saving and successful decorum
to rigidly splint multiple implants in a precise
manner is the Intraoral Welding Technique.3
Welding involves a metallurgical union process
that relies on base metal fusion, i.e. the constituent
metal of the structure, with or without the addition of
filler metal, to form the soldered joint.3 In intraoral
welding, a titanium bar is welded to the implant
abutments directly inside the oral cavity. It was
introduced by Hruska and Mondani3 in 1976.
Further it has been widely documented by Degidi
et al in 2006, who mentioned the creation of precise
and passive prosthetic structure by assembling the
framework directly inside the oral cavity.
Intraoral welding can join and support the
implants by the use of a titanium wire or bar that
is permanently connected to the implants. An
electric current for milliseconds is used to fuse the
titanium to the abutments. The welding procedure
is performed intraorally before the immediate
loading. Stabilization and fixation of the implants
allows immediate loading and prosthesis insertion (provisional or definitive) to occur on the same
day of the surgery. By inserting a prosthesis with
adequate retention and stability the same day as
the surgery, patient complaints and discomfort
can be avoided or minimized. The immediate
stability, which is a result of implant splinting can
also reduce the risk of failure during the healing
period. It can also eradicate the faults caused by
inappropriate making of impressions.4
Intraoral welding can be performed either with
a laser device - intraoral laser welding (ILW) or
by electric resistance welding – intraoral welding
(IOW). Electric resistance welding was introduced
by Pier Luigi Mondani5 in 1976 and then developed and perfected, and is based on the creation of
an electric arc between two electrodes under an
argon gas flux and it is called “syncrystallisation.’’6
Syncrystallization is the term used to describe the
union of two metallic surfaces through the sharing
of atoms constituting the crystal lattice in the joint
zone. Gordon7 discussed the probability of welding
metallic portions of dental prosthesis using laser
technology in 1967. According to many authors,8
laser technology is one of the best among all of
three welding techniques, which can be used
for different metals and it is the most effective
method for delivering thermal energy to small
areas as it permits the generation of a keyhole
that effectively concentrates the energy input
into one small area. Resistance to corrosion and
mechanical strength of the welded joint can also be improved with laser welding.7 Shielding gases
used in laser welding units shield the molten metal
from oxidation but there are some limitations to
welding such as porosity and cracks, which can
be reduced by vaccum welding. Carlo Farnaini
et al.(2014)9 reported that peak power is the
most significant parameter while determining the
penetration depth which is equal to pulse energy
per pulse duration. If the peak power is increased
too much, the temperature of the alloy exceeds to
the evaporation point, it will cause crater formation
on surface of the materials.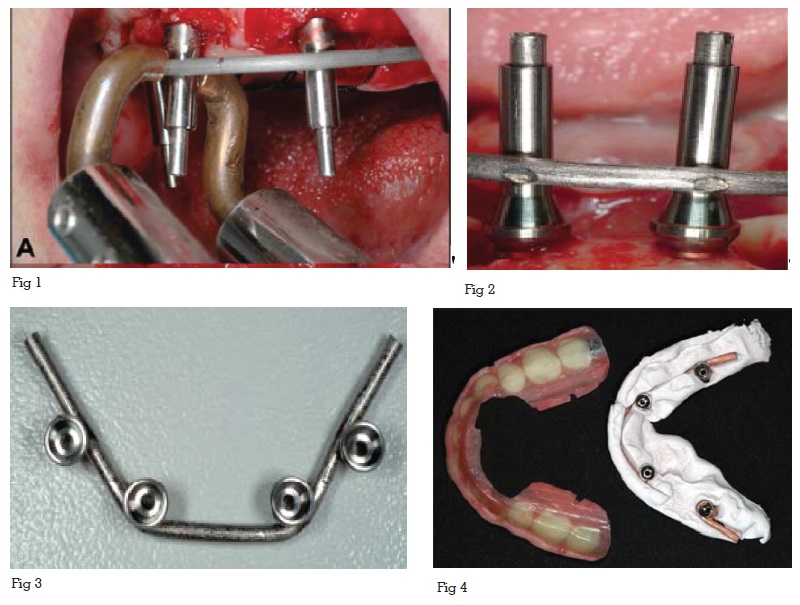
Historically, the welding machine was officially
introduced in the early 1970s, while the technical
description of this invention was only published
later in 1982.10 In the seventies COMEPRE Company
collaborated with Dr. Pier Luigi Mondani10 to
develop ‘’Syncrial’’ the first intraoral welding
machine allowing the welding by syncrystallization
of scialom needles by spot welding points, of
parts or of metallic implants also already firmly
implanted in the bone tissue.11 Initially, however, no
one except the inventor dared to use an electrical
device (Endoral welder) that had to reach a melting
point of 1678° C in order to solder –inside the oral
cavity - the ends of metallic artifacts placed in the
bone. Later Mondani’s technique was employed
at the Specialization School of Dentistry of the
University of Modena, where it was tested and
certified as safe, and reported that it does not
harm the tissues with which it comes into contact.
The “biocompatibility” of the soldering, which
occurs at 1678°C on the protruding and closely
set portion of the needles placed in living tissue,
is due to the fact that the electric current needs a
working time of just 2–3 milliseconds. This microtime,
combined with the calculated pressure of
the electrodes on the structures to be soldered,
prevents the diffusion of the tremendous heat
gradient beyond the welding point. Apart from
being a bad conductor, titanium also has low
thermal conductivity which is very similar to that of enamel.12
Nowadays Intraoral Welding devices are available
in various companies such as Dentsply, ITS Italy,
Swiss & Wegman etc. Recent Intraoral Welding
devices are based on the resistance spot welding
principle. They provide a stable and passively
fitting framework for temporary or durable
prostheses for immediate restorations – suitable
for immediate or late loading on the same day
of surgery.
After the implant site selection, implant are placed
with widely possible antero posterior distribution
using surgical template. Angulated abutments
are connected to the implants immediately after
the implant placement. First, a so-called welding
abutment, a titanium cylinder, is connected to each
abutment with a long pin screw. A 2.0-mm-diameter
bar made of grade 2 commercially pure titanium
is welded to the most distal abutment on the left
using an intraoral welding unit. The bar is then
adjusted with orthodontic utility pliers to passively
contact all the abutments. The whole welding
process is divided into three parts: Preparation,
Welding, and Cooling stage.13 In the Preparation
stage, two electrodes of the welding pincers are
placed on either side of the bar and the abutment,
both of which must be clean and free of surface
oxidation. The copper electrodes at the extremities
of the pincers are gently put into contact with
the parts to be welded and firm pressure is then
applied (Fig1). It is important to maintain complete
contact between the curved bar and the welding
abutment during the entire process. Firm and
constant pressure must be constantly applied
to ensure a perfect joint between the parts to be
welded. The presence of water or saliva does not
compromise the quality of the welded joint. The
surgical team and the patient must wear protective
goggles during the entire process.”
In the Welding stage, An electrical charge from a previously unloaded capacitor is transferred
to the copper electrodes of the welding pincers.
Electrical current which is supplied to the
electrodes instantly raises the temperature of
the two titanium components to fusion point (Fig
2). The process takes only 2 to 5 ms to carry out
and brings the core of the titanium parts to a
temperature of nearly 1,660°C. A barely perceptible
clicking sound can be heard during this phase.
This procedure is performed without the use of
any additional filler metal.
In the cooling stage, the titanium crystallizes. To
avoid crystallization of titanium, the bar and the
abutment must be kept under firm pressure and if
all of the instructions are followed properly, a solid
joint is formed. The only way the process can fail
is if there is inaccurate positioning of the titanium
components or if insufficient pressure is applied
during the welding and cooling stages. If either of
these occur, the joint obtained is very unstable and
fragile. After the welding, the prosthetic framework
is removed (fig 3) and its passivity is checked with
the Sheffield 1-screw test. The welding abutments
of the framework are screwed to analogs of the
angulated definitive abutments and are inserted
in cast model. Framework is finally refined to fit
the prosthesis (fig 4).
If more rigid structure is required or if titanium bars
are used with thin diameters, an additional bar
can be welded onto welded abutments, following
the exactly same procedure as for the first bar
removing the structure after each welding to check
for passive fit of the prosthesis.14
Bars can be welded in various ways
Advantage of intraoral welding procedure is to
create a very precise rigid framework quickly and
directly inside the oral cavity, when immediate
functional loading is planned.15 Rigid framework
splinting obtained by this technique, can limit
the micromovements in immediate loading
protocols and is indicated in partial and fullarch
prosthesis, which reduces the mechanical
stresses exerted on each single implant and
assure an optimal distribution of occlusal load
and decreasing the lateral forces on healing
implant. With this technique, time-costly laboratory
steps can be avoided, such as the creation of
a customized impression tray, while a passive
fit of the framework is easily obtained.16 When
implants are splinted together, partial and full
arch immediate restorations can be performed
under low insertion torque. This reduces the
micromovements of weaker implants and hence
in turn increases the osseointegration.17 No major
limitations have been reported to this technique.
“Unfortunately, there are more limits to
syncrystallisation and electric resistance welding,
as these are not effective on every kind of metal
and alloy, and these cannot be used on patients
with pacemaker. Among the techniques, laser
technology found to be the most efficient method
for delivering thermal energy to small areas. It
is one of the best fusion welding techniques for
different metals.18 This depends on the ability to
focus the light beam in a focal point. The best
advantage is that the weld process can usually be
performed exactly where it is required, that is, at
the level of an implant abutment.19 Moreover, the
procedure can be carried out directly on the master
cast, thereby eliminating the risk of inaccuracies
and distortions due to the duplication of the model
and the heat source, being a concentrated highpower
light beam, and minimizing the distortion
problems in the prosthetic pieces.20
The clinical use of the intraoral welding technique
to immediate load the implants surgically inserted with computer assisted surgery reported to be
a good treatment approach nowadays, which
allows the creation of an immediate and
passive provisional restoration that could limit
complications reported in the past and reduce the
intraoperative time with respect to the traditional
technique of intraoral welding.21
Titanium bars welded intraorally on prostheses is
now a widely proven technology and allows the
stabilization of fixed prostheses in edentulous
ridges that otherwise could not be rehabilitated.
The welded joint structure reported excellent
microstructural quality, with only minor porosity
detected at 50,000× magnification. Welded joint
between abutment and titanium bar after subjected
to functional loading showed no fracture or
radiographically detectable alteration, improving
the quality of the results,reducing the operative
time, and giving greater comfort to the patient.22