Obtaining consistent mandibular denture stability has long been a challenge for the dental profession. Atrophic ridges in particular is often associated with difficulties in providing successful denture. Stability of lower denture in such cases is usually the distinguishing factor between success and failure. Various conservative prosthodontic techniques have been implemented to improve denture stability in atrophic ridges. Neutral zone technique is long being used for the management of atrophic ridges. In severe cases where neutral zone is not effective, a combination of neutral zone along with sublingual crescent technique can be followed to obtain maximum stability. This paper highlights such a case where the mandibular denture stability was attained by the combination of the above techniques.
Key words: Neutral zone technique; sublingual crest technique; Sublingual crescents; Retention; Stability; Severely resorbed mandibular ridge.
The great challenge of a prosthodontist is the
rehabilitation of a completely edentulous patient
with good functional and aesthetic outcome. This is
even more challenging when the patient presents
with a severely resorbed residual alveolar ridge. The retention and stability of the mandibular
dentures in such cases are more dependent on the
impression procedures and the positioning of the
teeth in the neutral zone. The neutral zone concept
was first described by Sir Wilfred Fish in 1931.1,2
The neutral zone is the potential space between
the lips and cheeks on one side and the tongue on
other, that area where forces between the tongue
and cheeks or lips are equal. This concept is not
new but is less often practiced.3
In a severely compromised ridges, the stability can
be attained by positioning the teeth in the neutral
zone where as the retention can be achieved by
another conservative approach,the sublingual
crescent technique.4 Sublingual crescent
recorded in the lower denture provides effective
peripheral seal in the vulnerable anterior part of
the alveololingual sulcus resulting in excellent
retention in ridges with normal height while
satisfactory retention in compromised ridges,
where achieving retention is just a dream.5 This
article highlights a case of severely compromised
ridge rehabilitated using the combination of two
conservative techniques- sublingual crescent
technique and neutral zone concept.
A 65-year-old female patient presented with the
complaint of ill-fitting denture. History revealed her 30 years of edentulousness and on examination
it was evident that her mandibular ridge was
severely compromised and had epulis fissuratum.
In left mandibular sulcus due to this ill-fitting
denture. [Fig 1] She was advised to discontinue
her existing denture and later reviewed after two
weeks to assess the relief of symptoms. As there
was no relief the epulisfissuratum was surgically
excised. After the healing period, considering
her severely resorbed mandibular ridge and
the chances of recurrence of epulisfissuratum,
the treatment planned was the fabrication of
conventional complete denture combining two
conservative approaches- neutral zone technique
and sublingual crescent technique. This was to
attain maximum denture stability and retention
possible.
After the preliminary impression of the maxillary and mandibular arches were made, the cast
were poured and the special tray was fabricated
conventionally. In the mandibular arch, the
border moulding with the low fusing compound
(DPI Pinnacle,the Bombay Burmach Trading
Corporation Ltd, Mumbai) was first done in the
mylohyoid, retro mylohyoid and the distal extension
of the tray, initiated from one side followed by the
other side. Thickness was kept approximately 3mm
in the lingual borders to stabilize the tray. Buccal
and labial areas were then border moulded.
Sublingual crescent recording was initiated
using admix technique. The softened material
was added in layers over the borders of the tray
from premylohyoid area of one side to the other,
finally spanning the entire anterior lingual area
with the admix compound. The added compound
is then tempered in hot water and premoulded to
approximate shape of sublingual crescent with the
fingers. The special tray was placed in the mouth
and the patient was instructed to gently place the tongue against the lingual side of the tray handle.
In order to relieve the lingual frenum, the area
was moulded using low fusing compound. [Fig 2]
Secondary impression was made using zinc oxide
eugenol impression paste (DPI Impression paste,
The Bombay Burmach Trading Corporation Ltd,
Mumbai) [Fig 3] Maxillary border moulding and the
impression was made in the conventional manner.
The casts were poured to get the mandibular
master cast with the additional positive replica
of the sublingual crescent. [Fig4]
Jaw relation was recorded and the lower occlusal
rim was removed and a neutral zone record base
was fabricated using acrylic resin. [Fig 5] Admix
impression material was softened in a water bath
of 65°C and attached to the record base. The record
base was reheated and seated in the patients
mouth and was asked to perform the actions of
smiling, pursing the lips, sucking and tongue
movements to register a neutral position where
buccolingual forces are neutralized [Fig 6]. A
labial and lingual index with additional silicone
(elite HD+, Zhermach, Italy) was made over the
neutral zone record to guide the positioning of the teeth on the mandibular definitive cast limited to
neutral zone. [Fig 7] Admix impression material
was removed from the record base and the index
was replaced to establish the space of neutral
zone. Molten wax was poured in the space and
the teeth arrangement was done respecting the
index limits. [Fig 7 and Fig 8]
Waxed trial denture was checked intraorally for
esthetic, phonetics, occlusal vertical dimension,
centric relation, stability and retention. [Fig 9] Trial
denture was invested, processed, finished, and
polished. Denture was evaluated in the patient
for retention and stability. Patient was extremely
satisfied with the new prosthesis without any
discomfort. [Fig 10]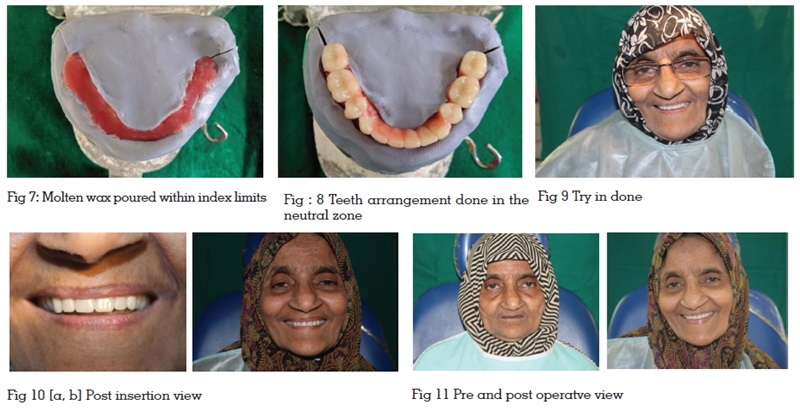
The factors affecting retention are highly
compromised in a severely compromised
mandibular ridge. Such patients are prone to
develop discomfort with the dentures made in the
conventional design. Although dental implants
can improve the retention of mandibular dentures, implant therapy is not viable in some patients
because of age, medical or economic constraints.5
Extending the anterior lingual flange of the lower
denture sublingually makes it possible to achieve
satisfactory retention in these severely resorbed
ridges. Lewis ET et al was the first to report about
the anterior sublingual area anatomy and some of
its problems and solution, which then he called it
as the genial tubercle or ‘sublingual fold space’.6
Friedman also has described the moulding of the
anterior lingual border of the impression but its
inadequacy has been mentioned by Lawson later
in his technique.7,8 The tongue movements may be
limited slightly due to the presence of sublingual
crescents which the patient gets adapted, if
extensions are proper. The patient can also perform
functional movements of the tongue sufficiently
without dislodging the denture.
From 1930s the neutral zone concept is known by
different terminologies like dead zone, stable zone,
zone of minimal conflict, zone of least interference,
zone of equilibrium, biometric denture space,
denture space, and potential denture space.9 In
1976, the term neutral zone was introduced by
Beresin and Schiesser which is now widely used.3
According to GPT 9 neutral zone is the potential
space between the lips and cheeks on one side and
the tongue on the other; that area or position where
the forces between the tongue and cheeks or lips
are equal.10 The dentures fabricated in this zone
will be more stable as during functional activities,
the forces exerted by the tongue are neutralized by
the lips and cheeks within the neutral zone. Admix
technique described by McCord and Tyson was
used to record the sublingual crescent and neutral
zone.11 It’s a combination of impression compound
and green stick (low-fusing) compound in the ratio
of 3:7. The mixing of a low-fusing compound with
the impression compound results in a low viscosity
material allowing for ease in manipulation of the
oral musculature. The admix material allowed
better flow and an accurate impression as it
removes the soft tissues folds easily and reduces any potential discomfort from the denture.12
Consistent mandibular denture stability has
long been a challenge particularly in atrophic
ridges. Various conservative approaches have
been implemented to improve the denture
stability in atrophic ridges including the neutral
zone technique which is long being used. So, in
cases where the neutral zone technique alone is
ineffective, its combination with the sublingual
crescent technique can be advocated to obtain
maximum retention. This case approves the success
of such a combined conservative approach.