Maxillofacial prosthetics is the branch of
prosthodontics concerned with the restoration and/
or replacement of stomatognathic and craniofacial
structures with prostheses that may or may not be
removed on a regular or elective basis.1
-GPT 9
Maxillofacial prosthesis is any prosthesis used to
replace part or all of any stomatognathic and/or
craniofacial structures.1
-GPT 9
Success in maxillofacial prosthetics depends on the
full cognizance of the principles that underlie facial
harmony, anchorage and retention, weight bearing
and leverage, durability, tissue compatibility and
tolerance.
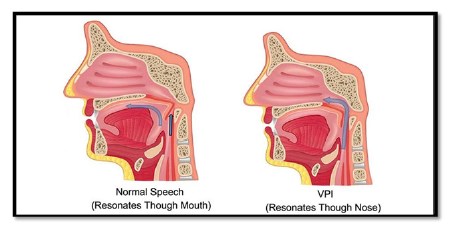
The velopharynx is a dynamic anatomic structure
which is essential for normal breathing, eating
and speech. The soft palate acts as a separator
between the oral and nasal cavities. Impairment of
velopharyngeal function can be caused by either
insufficiency or incompetency.
1. Speech aid prosthesis- a removable
maxillofacial prosthesis used to restore an
acquired or congenital defect of the soft palate
with a portion extending into the pharynx to separate the oropharynx and nasopharynx during
phonation and deglutition, thereby completing the
palatopharyngeal sphincter.(GPT9)1
2. Palatal lift prosthesis - a maxillofacial
prosthesis that elevates the soft palate superiorly
and aids in restoration of soft palate functions that
may be lost because of an acquired, congenital
or developmental defect.
Definitive palatal lift prosthesis- is usually made
for patients whose experience with a diagnostic
palatal lift has been successful, especially if
surgical alterations are deemed unwarranted.
Interim palatal lift prosthesis- is usually made as
a diagnostic aid to assess the level of possible
improvement in speech intelligibility. (GPT 9)1
3. Obturator -a maxillofacial prosthesis used to
close a congenital or acquired tissue opening,
primarily of the hard palate and/or contiguous
alveolar/soft tissue structures (GPT-7)2
Speech, as formulated, executed, perceived and
decoded, is unique to humans. The production of
speech requires the selective modification and
control of an outgoing airstream through the
complex and skilled coordination of more than
100 muscles within the respiratory, laryngeal,
velopharyngeal and oral mechanisms. This
intricate process begins within the CNS, but also
relies on PNS.
Kantner and West divided speech into 5
components:-
Chierici and Lawson added a sixth component
The successful and acceptable production of
speech depends on the successful performance
of these factors.
Respiration: speech begins with brief inhalation
followed by extended expiration, during which
pulmonary air interacts with resonating tubes and
chambers in the throat, mouth, nose an cranium
to produce audible speech signal for speech
to be produced, alveolar pressure must exceed
atmospheric pressure so that an outward flow of
air will occur.
Phonation: vocal folds and the associated
laryngeal musculature play a vital role in speech
production. For unvoiced sounds, air from the lungs
passes through an open larynx and is modified
by downstream articulatory structures to produce
speech sounds that are periodic in nature. For
voiced sounds, air from the lungs sets adducted
vocal folds into vibration, which creates a periodic
sound wave that is selectively resonated and
filtered within the vocal tract.
Resonation: the sound produced at the level of
the vocal folds is not the final acoustic signal that
is perceived as speech. The pharynx, oral cavity
and nasal cavity act as resonating chambers by
selectively filtering some frequencies and damping others, thus refining tonal quality.
Articulation: articulation occurs when resonated
sounds reaches the oral cavity. The sound wave are
formed into speech by the action of the moveable
articulators, including the mandible, tongue, lips
and soft palate against the immoveable articulator
structures including the hard palate, alveolar
ridge and teeth. Tongue is considered the most
important articulator.
Neural integrity: speech is integrated by the CNS
at both peripheral and central levels.
Mac Neilage and DeClerk stated that at least
17000 different motor patterns are required during
speech.
Audition: ability to receive acoustic signals, vital
for normal speech. Hearing permits reception and
interpretation of acoustic signals and allows the
speaker to monitor and control speech output.
Of the 6 components of speech, resonance and
articulation are the most relevant in maxillofacial
prosthesis and are closely related.
Resonance disturbances are basically of 4 forms
Mostly in patients with acquired mandibular
defects.
The velopharyngeal complex is divided into various
anatomical components: soft palate, posterior
pharyngeal wall, lateral pharyngeal wall.
Velopharyngeal closure is attained by synchronous
and sphincteric movements of the entire muscle
complex.
Velopharyngeal mechanism is a precisely
coordinated valve formed by several muscle
groups. At rest, the soft palate drapes towards
so that the oropharynx and nasopharynx are open
and coupled to allow normal breathing through
the nasal passage.
During speech, when velopharyngeal closure
is required, 4 patterns of closure is exhibited
[Skolnick et al.]
Classification of velopharyngeal defects
According to Taylor,
Palatopharyngeal insufficiency: when some or
all of the anatomic structure of the soft palate is
absent.
Palatopharyngeal incompetence: soft palate is of
adequate dimensions,but lacks movement because
of disease or trauma affecting muscular and/or
neurologic capacity.
Palatopharyngeal inadequacy: includes
incompetence and/or insufficiency but may also
suggest a reduction or absence of pharyngeal
wall function.
1. Palatopharyngeal inadequacy
Type of obturator
Immediate surgical obturation is most useful in
dentulous patients, where the entire soft palate
has to be resected. The principle advantage of
using immediate surgical obturators for soft palate defects is support and retention of the surgical
packing. Some disadvantages are, Firstly, the
drape of the intact soft palate precludes from
obtaining an impression of the nasopharynx,
where the normal velopharyngeal closure occurs
and where the surgical obturator should be
located. Secondly, functional movements of the
velopharyngeal mechanism cannot be recorded
either prior to or during surgery. Thirdly, the
pharyngeal tissues which are peripheral to the
defect will usually exhibit little movement during
function in the immediate postoperative period.
Fourthly, the extent of tumours in this region is
more difficult to visualize; hence, it is more difficult
to delineate the surgical margins presurgically.
Delayed surgical obturation: In edentulous
patients, or in patients with limited medial or lateral
posterior border resections, a delayed obturation
may be the treatment of choice. In edentulous or
partially edentulous patients, consideration should
be given to attachment of the delayed surgical
obturator to the existing maxillary complete or
partial denture
Patients exhibiting considerable movement of
the residual velopharyngeal complex during
function have excellent prognosis for achieving
normal speech with prosthesis. The obturator
is attached to a conventional prosthesis. If the
patient is dentulous, a removable partial denture
framework retains the obturator. The obturator
should be rigid. Therefore, it does not attempt to
duplicate the movements of the soft palate. It is
a fixed platform of acrylic resin, which provides
surface contact for the remaining musculature of
the velopharyngeal mechanism during function. If
the lateral and posterior pharyngeal walls exhibit
normal movement, a space will exist between these
structures and the obturator when these tissues
are at rest. This space permits breathing through
the nasal cavity. Subtelny et al., reported that a group of patients who could not speak successfully
and had restorations with pharyngeal sections
that extended below the palatal plane. Contact
between the palatal extension section and the
dorsum of the tongue was observed
2. Palatopharyngeal insufficiency
Types of pharyngeal obturators [According to
Sharry]
3. Palatopharyngeal incompetence
Types of palatal lift prosthesis
Prosthetic treatment with a palatal lift prosthesis
was first reported by Gibbons and Bloomer.
This type of prosthesis is especially useful for
patients with velopharyngeal incompetence. The
objective is to displace the soft palate to the level
of normal palatal elevation,thus enabling closure
by pharyngeal wall action. If the length of the
wall is insufficient to effect closure after maximal
displacement, the addition of an obturator behind
the displaced soft palate may be necessary.6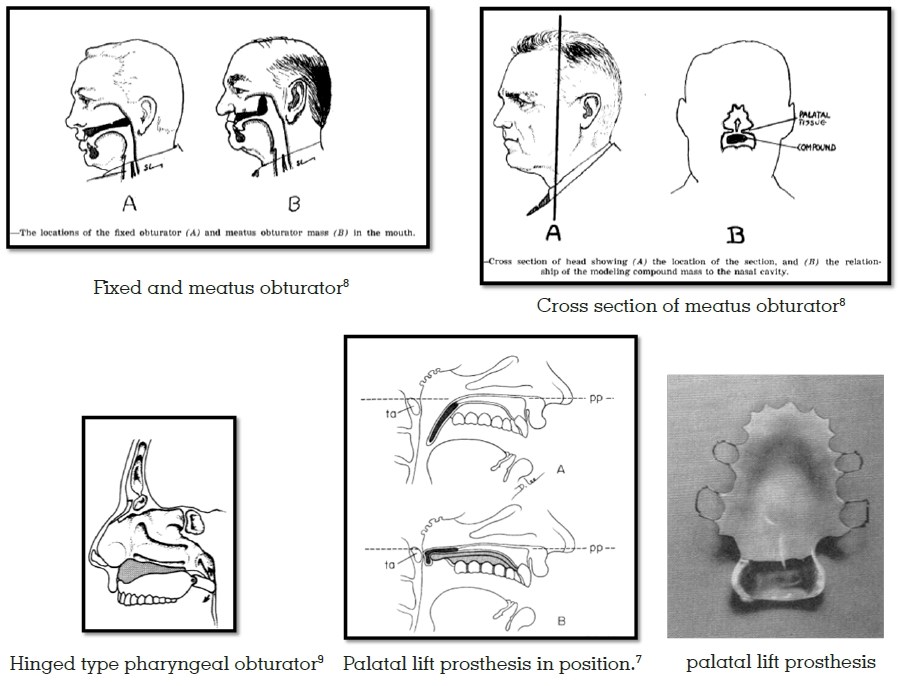
The primary objective in each case would be to
construct a prosthesis which will restore the defect,
improve aesthetics and thereby benefit the morale
of patient. The improvements in aesthetics and
function are not only essential for the patient’s
physical well being, but they also contribute to
his/her mental attitude.