Dental implants represent one of the most successful treatment modalities in dentistry1. Although high survival rates of implant supporting prosthesis have been reported , failure do occur due to bone loss in the range from 5 to 8% for routine procedures and up to 20% in major grafting cases after at least 5 years of function1,2. Achieving primary stability is of greatest importance, at the time of implant placement by new bone apposition at the bone– implant interface. A rigid mechanical engagement of implant within the host bone, with limited micromotion at the interface is the most critical factor for successful osseointegration. . Implant stability is estimated at two different stages Primary and Secondary. Primary stability of an implant is the absence of mobility in the bone bed upon insertion of the implant and mostly comes from mechanical interaction with cortical bone. It is also named as -Mechanical Stability which is the result of compressed bone holding the implant tightly in the bone.. Secondary implant stability is developed from regeneration, remodelling of the bone and tissue around the implant after insertion and is affected by primary stability. Implant instability with relative displacements above 50-150μm3 could result in fibrous encapsulation with resultant failure. It is of utmost importance to be able to assess implant stability at various times and to project a long term prognosis for successful therapy. The review focuses on different methods used for evaluation of implant stability and recent advances.
Osseointegration is a direct bone anchorage to
an implant body which can provide a foundation
to support prosthesis.4,5 Branemark defined it as
“A direct connection between living bone and a
load-carrying endosseous implant at the light
microscopic level.”.A rigid fixation of implant within
the host bone, with absence of micromotion at the
interface is the most critical factor for successful
osseointegration. Implant stability is a requisite
characteristic of osseointegration. Without it, longterm
success cannot be achieved.
Continuous monitoring of implants in a quantitative
and objective manner by setting up experimental
methods is important to determine the status of
implant stability. The majority of implant losses
may be explained as biomechanically induced
failures, since low primary implant stability, low
bone density, short implants and overload have
been identified as risk factors1. Hence, achievement
and maintenance of implant stability are preconditions
for a successful clinical outcome with
dental implants.
Dental implant stability can be divided into
primary and secondary components. Primary
stability refers to the initial mechanical bracing
of the implant in bone and absence of any
micromovement, while secondary stability refers
to successful osseointegration of the implant with the surrounding bone.7
Achieving Primary stability is of utmost importance,
at the time of implant placement.
If an implant is not sufficiently stable at the time
of implant placement, micro-motions may occur,
normal healing process may then be disrupted
and a fibrous tissue capsule may form, resulting
in clinical mobility and subsequent implant failure.
Bone quantity and quality, surgical techniques
including the skill of the surgeon, implant
(geometry,length, diameter,drill size and surface
characteristics) are major factors affecting primary
stability8. Bone quality and quantity modification
can be done by augmentation procedures or by
use of bone grafts but the quality of bone is one
parameter were in the clinician has limited control
as compared to other parameters such as implant
design and surgical procedure. Using a smaller size
drill in diameter than implant produces compressive
stress around implant-tissue interface,resulting in
compression of the bone in the implant vicinity
when implant is surgically driven. Such stresses
are beneficial in terms of attaining good primary
stability, but if these stresses surpasses optimum
levels than it may result in local ischemia of bone
and necrosis8. Change in implant stability after
insertion is due to regeneration and remodelling
of bone at implant tissue interface is considered
to be secondary stability. Secondary stability is
a biological stability. It involves regeneration
and remodelling of bone and tissue around the
implant over a period of time. It depends upon
primary stability, bone formation and remodelling.
Complete bone-implant contact rarely occurs and
clinically observed osseointegration corresponds to
approximately 80% of bone contact. Though, more
than 60% of bone-implant contact is considered
to be adequate for implant stability. There are
various methods which have been suggested in
literature to measure implant stability.7
Various methods to check implant stability as
categorized as follows:-
Invasive or Destructive methods
Non Invasive or Non Destructive Methods
1. Histologic or histomorphologic analysis
This method quantitatively assess the bone
contact and bone area from a dyed specimen of
the implant and peri-implant bone. Due to invasive
and destructive nature of the technique it is limited
to non-clinical and experimental studies.8,10
2. Tensional test
The strength of the implant was earlier measured by detaching the implant plate from the supporting
bone. It was later on modified by applying lateral
load to cylindrical implant fixture. However there
were difficulties in translating the test results to
any area independent mechanical properties.11
3. Push out / pull out test
This test evaluates the healing capabilities at the
bone implant surface. In this test, a cylinder type
implant is placed transcortically or intramedullary
in bone and then removed by applying a force
parallel to the interface. The maximum load
capability is defined as the maximum force
displacement. However the push out pull out tests
are only applicable for non-threaded cylinder type
implants, whereas most of clinically available
fixtures are of threaded design and then interfacial
failures are solely dependent on shear stress
without any consideration for either tensile or
compressive stresses.11,12
4. Removal torque analysis
In this test an implant is considered stable if
the reverse or unscrewing torque is > 20Ncm.
Osseointegrated implants resist this torque while
failed implant unscrew. However, the drawback is that at the time of abutment connection the
implant surface in the process of osseointegration
may fracture under the applied torque stress.
This test doesn’t give a clear clarity of degree of
bone healing or bone formation around implant
but provides result only about osseointegrated or
failed implant bone interface.8,11,13
1. The surgeon’s perception
One method of trying to evaluate primary stability
is quite simply the perception of the surgeon. It
is based on the cutting resistance and seating
torque of the implant during insertion. A perception
of “good” stability may be heightened by the
sensation of an abrupt stop when the implant is
seated. However, this type of measurement can
only be made when the implant is inserted, it
cannot be used later, for example, before loading
the implant.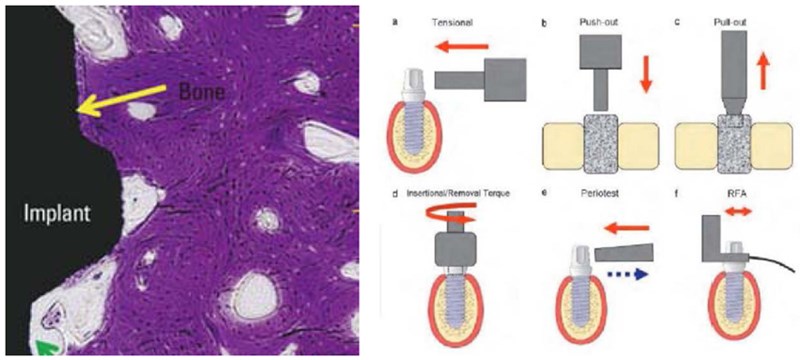
2. Imaging techniques
Various radiographic and imaging techniques
are used to clinically evaluate the quality and quantity of bone before the placement of implant
fixture. The most common methods for assessing
bone implant integration analysis are periapical
radiography,panoramic radiography,computed
tomography (CT),Cone beam computed
tomography (CBCT) etc.
3. Cutting – torque resistance analysis
It was originally developed by Johansson and
Strid and later improved by Friberg et al. The
energy required to remove a unit volume of bone
is significantly correlated with bone density
and quantifies bone hardness during implant
osteotomy at the time of implant placement. It
provides information in determining an optimal
healing period in a given arch location with a
certain bone quality. Longitudinal data cannot be
collected to evaluate bone quality changes after
placement of implants.14
Limitations
4. Insertion torque measurement
Insertion torque values have been used to measure
the bone quality in various parts of the jaw
during implant placement.15,16 It is a mechanical
parameter generally affected by a surgical
procedure, implant design and bone quality at
the implant site.17 A disadvantage of this method
is that the insertion torque varies depending on the
cutting properties of the implant and the presence
of fluid in the preparation. It can only be used
during implant placement and not possible at
later stages of the treatment.
5. Reverse torque test
It was proposed by Roberts et al14,19 and developed
by Johannson and Alberktsson. It evaluates the
secondary stability of the implant. It measures the torque threshold where bone implant contact was
destroyed. Measurement of lateral mobility is more
useful than measurement of rotational stability
as an indicator of successful treatment result. It
cannot quantify the degree of osseointegration
as threshold limits vary among patients, implant
material, bone quality and quantity. The studies
showed, the stress of applied torque may in itself
be responsible for the failure.20
6. Seating torque test
Like insertion torque, the final seating torque gives
some information about the primary stability of
the implant when the implant reaches its final
apico-occlusal position. It is done after implant
placement.16
7. Percussion test
A simple method used to measure the level
of osseointegration. This test is based upon
vibrational acoustic science and impact response
theory. The clinical judgement of osseointegration
is based on the sound heard upon percussion with
a metallic instrument. A clearly ringing ‘crystal’
sound indicates successful osseointegration
whereas a ‘dull’ sound may indicate absence of
osseointegration. This method mostly relies on the
doctor’s experience level and subjective belief.
Therefore, it cannot be used experimentally as a
standardized testing method.14,17
8. Periotest
Quantifies the mobility of an implant by measuring
the reaction of the peri-implant tissues to a defined
impact load. The periotest was introduced by
Dr.Schulte to perform measurements of the damping
characteristics of the periodontal ligaments, thus
assessing the mobility of natural tooths.20,21 It uses
an electromagnetically driven and electronically
controlled tapping metallic rod in a hand piece.
Periotest value range from -8 (low mobility) to +50
(high mobility). Response to a striking” is measured
by a small accelerometer incorporated into the
head. The reliability of this method is questionable because of poor sensitivity,susceptibility to many
variables22. The factors that influence the periotest
value are the quality of the hard tissue in the
region of the implant, so that no specific values
can be deemed as appropriate for higher or lower
degrees of integration. The measurements are
significantly affected by direction and position.
It measures implant stability and bone density at
the time of implant placement and post surgical
placement of the implant.
9. Pulsed oscillation wave form
Kaneko23 described the use of a pulsed oscillation
wave form (POWF) to evaluate the properties
of mechanical vibrations of the bone-implant
interface using forced excitation of a steady state
wave. POWF is based on estimation of frequency
and amplitude of the vibration of the implant
induced by a small pulsed force.
A multi frequency pulsed force of about 1 kHz is
applied to an implant by lightly touching it with two
fine needles connected with piezoelectric elements
(contained in an accous to electric driver AED,
and acoustoelectric receiver AER). It is used for
in-vitro and experimental studies. The sensitivity
of the POWF test depended on load directions
and positions
10. Resonance frequency analysis
In 1998, Meredith25 suggested a non-invasive
method of analyzing implant stability and bone
density at various time periods using vibration
and a principle of structural analysis. This method
has L-shaped transducer that is tightened to the
implant or abutment by a screw. The transducer
provides a high frequency mechanical vibration
and record the frequency and amplitude of the
signal received.
The transducer comprises of two ceramic elements,
one of which is vibrated by a sinusoidal angle
(5 – 15 kHz ) while the other serves as a receptor.
The transducer is screwed directly to the implant body and shakes the implant at a constant input
and amplitude starting at a low frequency and
increasing in pitch until the implant resonates.
High frequency resonance indicates stronger boneimplant
interface.
RFA has been widely used for clinically assessing
osseointegration, as well as for prognostic
evaluation. The most recent version of RFA is a
wireless gadget. A metal rod is attached to the
implant with a screw connection. The rod has a
small magnet attached to its top that is stimulated
by magnetic impulses from a handheld electronic
device. The rod mounted on the implant has two
fundamental resonance frequencies, it vibrates
in two directions, perpendicular to each other.
One of the vibrations is in the direction where
the implant is most stable and the other is in the
direction where the implant is least stable
11. Electronic Technology Resonance Frequency
Analysis (Osstell)
It was the first commercially available product
for measuring implant stability. The electronic
technology combines the transducer, computerized
analysis and the excitation source into one
machine.
Implant stability quotient (ISQ) is the measurement
unit (ISQ of 0 to 100 ) used. When used at the time
of implant placement it provides baseline reading
for future comparison and post-surgical placement
of the implant.
Vibration tests are based on the assumption that
the resonance frequency is directly related to the
stiffness of the bone–implant interface, and of
the surrounding bone: they act like two springs in
series, therefore the softer one plays the greatest
influence26. As a general rule, high values of
resonance frequency are produced by successfully
integrated implants, while low values may be signs
of ongoing mobilization and/or marginal bone
loss. Caution has been expressed by the European
Association of Osseointegration (EAO), since it has been realized that Resonance Frequency
Analysis (RFA) is affected not only by bone tissue
characteristics, but also by the effective implant
length, diameter, and surface characteristics. This
is the reason why no established normative base
on RFA is available yet, and the trend of resonance
frequency versus time is thought to be significant,
rather than its absolute value, measured at a
certain time step.
Implant stability quotient (ISQ) is the measurement
unit (ISQ of 0 to 100 ) used.27 When used at the
time of implant placement it provides baseline
reading for future comparison and post-surgical
placement of the implant.
12. Magnetic Technology Resonance Frequency
Analysis (Osstell Mentor)
The transducer has a magnetic peg on the top and
is fixed to implant or abutment. On activation by
magnetic resonance frequency probe the pegs
activated, which vibrates and induces electric
volt sample by magnetic resonance frequency
analyzer. Values are expressed as ISQ of 0 – 100.
At the time of implant placement it provides base
line reading for future comparison and postsurgical
placement of the implant.
However this method is expensive and technique
sensitive as it requires respective transducer and
magnetic peg. It should maintain a distance of 1
– 3 mm, angle of 900 and should be 3 mm above
the soft tissue otherwise the measured value will
be affected.28,29
13. Modal Analysis
Modal analysis is also known as vibration analysis.
It measures the natural frequency or displacement
signal of a system in resonance, which is initiated
by external steady – state waves or a transient
impulse force.
It can be performed in two models Theoretical
and experimental.
The theoretical modal analysis includes finite
element analysis. It investigates vibrational
characteristics of objects. It is done to calculate
stress and strain in various anticipated bone levels.
It is used in clinical studies and experimental
studies.
The experimental modal analysis is a dynamic
analysis. It measures natural characteristic
frequency, mode and attenuation- via vibration
testing. It is used in non-clinical studies in-vitro
approach and provides reliable measurements.30
The description of various techniques in the above
literature states that the advanced and tests and
equipments may play a more prominent role in
the assessment of implant stability as compared
to conventional methods. The ability to monitor life
expectancy of an implant and its osseointegration is
a valuable diagnostic and a clinical tool. Although
RFA has attracted considerable scientific interest
in recent years, it can also be used to evaluate the
effect of early and delayed loading assess stability
over a period of time and early diagnosis of implant
failure. However, more research is necessary to
invent an accurate instrument which will help
gauge the implant stability.