Since the development of ruby laser by Maiman in 1960, a variety of studies on the potential applications of lasers in dentistry have been conducted. Many applications like computer aided design and rapid prototyping technology, and study of occlusion in complete dentures using threedimensional laser scanner have been developed. Its applications range from fixed Prosthodontics, treatment of dentinal hypersensitivity and to surface treatment of base metal alloys. Today it even extends to the fields of dental implantology and maxillofacial Prosthodontics. This article reviews and summarises various studies of laser applications in Prosthodontics.
Key words: LASER, Complete Denture, CAD/CAM, Impression, Crown Preparation, Welding, Dental Implants, Maxillofacial Prosthesis.
Light is an integral part of our life. The early 20th century saw one of the greatest inventions in science & technology, in that LASERS (Light Amplification by Stimulated Emission of Radiation) went on to became a gift to health sciences. A laser is an instrument that produces a very narrow, intense beam of light energy (electromagnetic radiation) through a process called stimulated emission. Albert Einstein is usually credited for the development of the laser theory. He was the first one to coin the term “Stimulated Emission” in his publication “Zur Quantentheorie der Strahlung”, published in 1917 in the “Physikalische Zeitschrift”1.
Their application range from a simple television remote to computer devices such as laser mouse, presentations, CD ROMs, DVD ROMs, Astronomy and communication application, war machines, guns and tanks, cutting and welding in metallurgy industries, Robotics and even in toys.
The use of lasers for treatment has become a common practice in the medical field. Theodore Harold Maiman is generally credited for building the first working ruby laser and operating it for the first time on May 16, 1960 at the Hughes Research Laboratory in Malibu, California. MASER a microwave amplifier by Charles H.Townes, P.Gordon et al became the basic principle for laser pumping. This set the stage for a “snowball effect” which would lead to the development of many laser systems, which we utilize in healthcare today. The application of laser to dental tissues was reported by Stern, Sognnaes and Goldman et al. in 1964, describing the effects of ruby laser on enamel and dentine with a disappointing result. However, with the recent advances and developments of wide range of laser wavelengths and different delivery systems, researchers suggest that lasers could be applied for the dental treatments too.1
Currently, numerous laser systems are available for dental use. Neodymium-doped: Yittrium- Aluminium-Garnet (Nd: YAG), carbon dioxide (CO2) and semiconductor diode lasers have already been approved by the United States Food and Drug Administration for soft tissue treatment in oral cavity. The Erbium doped: Yttrium-Aluminium- Garnet (Er: YAG) laser was approved in 1997 for hard tissue treatment in dentistry2.
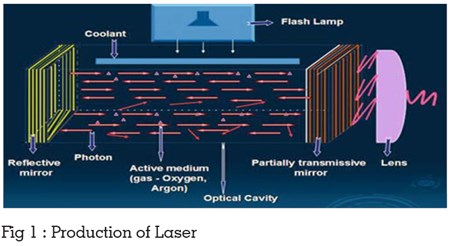
The basic components of a laser are straight forward and are always similar regardless of the type of equipment. They include an active lasing medium within an optical cavity (resonator) and a pumping source (energy source). The optical cavity consists of two mirrors placed on either side of the laser medium. Due to this arrangement, photons resulting from the stimulated emission will form a continuous avalanche process. As long as the pumping energy maintains the population inversion in the active medium, more stimulated photons are created thus producing energy. The energy is absorbed and emitted in the resonator and with the aid of mirrors, is reflected and resonates within this chamber, and ultimately produces laser light. Because one of the mirrors is partially transmissive, some of the laser energy escapes at one end of the device into a delivery system. Consequently; a laser is just a source to generate a high energetic beam of light, which is monochromatic, collimated and coherent (Fig 1).
In medical, the photo thermal effect is in the range of m sec to sec of irradiation time. The light energy is converted into thermal energy, which is locally cooled by water that irrigates the irradiated and surrounding tissue. As the temperature increases at the surgical site, the tissues can be warmed up to (37-50°C), coagulated (60-70°C), welded (70-90°C), and vaporized (100-150°C). If the laser energy continues to be absorbed by the tissue, carbonization occurs (>200°C) and with it the possibility of significant tissue damage. Consequently, both target and surrounding tissues can be subjected to these harmful effects.3
The laser classification system is based on the
probability of damage occurring.
Class I- (< 39mw) Exempt; pose no threat of
biological damage.
Class II- (< 1 mw) The output could harm a person
if he were to stare into the beam for a long period
of time. The normal aversion response or blinking
should prevent you from staring into the beam.
No damage can be done within the time it takes
to blink.
Class IIIA - (<5OOmw) Can cause injury when
the beam is collected by optical instruments and
directed into the eye.
Class IIIB - (<5OOmw) Causes injury if viewed
briefly, even before blinking can occur.
Class IV - (> 5OOmw) Direct viewing and specular
and diffuse reflections can cause permanent
damage including blindness.
PROTOTYPING AND CAD/CAM TECHNOLOGY:
The term rapid prototyping (RP) refers to a class
of technologies that can automatically construct
physical models from Computer-Aided Design
(CAD) data. These “three dimensional printers”
allow designers to quickly create tangible
prototypes of their designs, rather than just twodimensional
pictures. Such models have numerous
data.
In addition to prototypes, RP techniques can also
be used to make tooling (referred to as rapid
tooling) and even production-quality parts (rapid
manufacturing).A software package slices the CAD
model in to a number of thin (eg.0.1mm) layers,
which are then built up one atop another. Rapid
prototyping is an additive process, combining
layers of paper, wax, or plastic to create a solid
object.
In contrast, most machining processes (milling,
drilling, grinding, etc.) are “subtractive”processes
that remove material from a solid block. RP’s
additive nature allows it to create objects with complicated internal features that cannot be
manufactured by other means.5,6
Laser Rapid Forming of A Complete Titanium
Denture Base Plate:7 This technique uses the
combination of the CAD/CAM and LRF (Laser
Rapid Forming) methods for forming the titanium
plate of a complete denture. Laser scanner, reverse
engineering software, and standard triangulation
language (STL) formatted denture base plate and
sliced into a sequence of numerical controlled
codes.
The denture plate will be built layer-by-layer, on
the LRF system. After the traditional finishing
techniques, this denture plate will be acceptable
for use in patients.
After fabrication of new dentures the occlusion
can be examined and studied with the help of
laser scanner technique and three-dimensional
reconstruction. The laser scanner scans the
occlusion of the dentures fabricated, then the
scanned image is used to fabricate the three
dimensional structure by three-dimensional
reconstruction. The relationship between the
parameters of balanced occlusion can also be
analyzed.
Several studies have made comparisons in the
dimensional accuracy of different elastomeric
impression materials. Most have used two
dimensional measuring devices, which neglect
to account for the dimensional changes that exist
along a three-dimensional surface.
The scanning laser three-dimensional (3D) digitizer
can delineate x, y, and z coordinates from a
specimen without actually contacting the surface.
The digitizer automatically tracks and coordinates
with precision and stores data as the number of points on a surface with a resolution of 130 mm
at 100 mm. These exacting features suggest that
the laser digitizer might accurately and reliably
measure the dimensions of dental impression
materials while avoiding subjective errors.
The image is built up and landmarks identified
which allow superimposition of the images and
enable the differences between two similar images
to be calculated. The 3D laser captures complex 3D
texture-mapped models and they are exported into
a 3D (Scan Surf) software application where it is
built and triangulated into a 3D meshwork image of
the object. The scanning process is accomplished
within a minute whereas the software analysis
takes much longer. The software superimposes
the two objects by either registering landmarks
or by registering as iterative closest point (ICP).
This finds an optimal fit between the two surfaces
and in effect acts as a reference area. Once
superimposed, the difference of the two surfaces
is calculated as the shortest distance of each point
on one object surface from a second object surface,
within a range of 0.5 mm. Three-dimensional
digitizers will eventually become less expensive,
require less maintenance, track faster, and be
available with more standardized software.
I) TISSUE MANAGEMENT:
Crown lengthening:9 This is a procedure when
inadequate crown height is present for crown
restoration an adequate crown height is created
by removing required gingival soft tissue. With the
help of the lasers soft tissue crown lengthening can
be done without raising a flap. By its thermal effect
the laser seals vascular and lymphatic vessels
at the same time it vaporize the excess gingival
tissue. Since no flap was required for this surgery,
sutures were not necessary and the wound healed
by secondary intention.
Advantages:
II) CROWN PREPARATION:10
Crown preparation with lasers a debated topic
still. There are no conclusive studies yet showed
the use of lasers for crown preparation purposes.
But still some commercial companies say that they
can be used. The following is the details what
these companies say:
Er, Cr: YSGG laser is used most commonly now.
It uses hydrokinetic technology (laser-energized
water to cut or ablate soft and hard tissue).Because
of this mechanism local anesthesia is not required
in many cases, making this more comfortable
procedure for the patient, and of course, saving
time and anesthetic use by the patient.
The laser hand piece resembles a high-speed
hand piece but with fiber-optic tips instead of a
bur, which directs the laser energy at a focal point
approximately 1-2 mm from the tissue surface.
The crown preparation should be started on
maximum setting for cutting enamel (6W,90%
air,75% water),started with a defocused mode for
30 seconds to 1 min for anesthesia of tooth.
While placing the gingival margin setting will be
reduced 1.25 W, 50% air, 40% water to control the
cutting tip, for the purpose of accuracy.
To finish with the interproximal, buccal, lingual/
palatal reduction cuts will be performed with the
dentin settings 4W, 65% air, 55% water. The laser has to be reset at 2.25 W, 65% air, 55% water
to finish the buccal cusp overlay, and the final
margination of the proximal and lingual surfaces.
Advantages:
Disadvantages:
LASER WELDING:
The removable partial dentures defect can be
repaired by the use of pulsed laser with relative
low average out power. This is known as a precise
and rapid joining method, but its success depends
on the control of many parameters.
Eg: For Co-Cr alloy frameworks:
The welding parameters were determined for each
defect type and working step (fixing, joining, filling,
planning). Adequate combination of pulse energy
(6-14 J), pulse duration (10-20ms) and peak power
(600- 900 W) depending on the working stage
improves the success of the welding procedure.
FOR STERILIZATION OF SOCKET:
In immediate implant dentistry after extraction of
tooth,sockets can be sterilized immediately without
inducing pain and any infection.
IN CASE OF PERI- IMPLANTITIS:
Since the laser does not transmit damaging heat,
it can be utilized to vaporize any granulation
tissue as well as clean the implant surface in
periimplantitis cases. This procedure eliminated
the acute state of peri-implantitis, resulting in positive GTR, and allowing the patient extended
use of the implant.
TO DEBRIDE THE IMPLANT SURFACE:
Miller Robert has shown that treatment of the
contaminated implant surface by mechanical
and chemotherapeutic means has met with mixed
success. Development of a laser system operating
at 2780 nm and using an ablative hydrokinetic
process offers the possibility for more efficient
decontamination and debridement. Laser ablation
using the Er: Cr: YSGG laser is highly efficient at
removing potential contaminants on the roughened
implant surface while demonstrating no effects on
the titanium substrate.
New advances in rapid prototyping technologies
have demonstrated significant advantages
compared to more conventional techniques for
fabricating facial prosthesis. The use of selective
laser sintering technology is an alternative
approach for fabricating a wax pattern of
maxillofacial prosthesis. This new approach can
generate directly by prototyping and reduce laborintensive
laboratory procedures.
SLS (SELECTIVE LASER SINTERING):
The SLS (Selective Laser Sintering) is a method of
computer aided designing using mainly the laser.
In this method models are generated directly from
3-D computer data then converted to STL files,
which are then sliced in to thin layers (typically
about 0.1 mm/0.004 inches) using the associated
computer software. The laser sintering machine
produces the models on a removable platform by
applying incremental layers of the pattern material.
For each layer, the machine lays down a film of
powdered material with an accurate required
thickness, again a fresh film of powder is laid
down, and the next layer is melted with exposure
to the laser source. This process continues, layer
by layer, until the pattern is completed.
ADVANTAGES:
LIMITATIONS OF LASERS:14
The laser technology has been widely used in
dentistry on both hard and soft tissues in various
treatment modalities. However, lasers have got
their own limitations specifically being technique
sensitive. It has never been the “magic wand” in the
field of medicine or dentistry but been beneficiary
as an adjunct with other procedures used for the
treatment. In the future laser dentistry can be more
brighter with going on further research. Even now
Lasers are blessing in disguise if used efficaciously
and ethically. As Aaron Rose Says, “In right light
at right time everything is extraordinary.”