Orofacial clefting is one of the most prevalent congenital defects. The rehabilitation of such cases poses technical, economical as well as emotional difficulties. A feeding obturator device, obturates the cleft palate, restoring the separation between oral and nasal cavities.
The children born with orofacial clefting has to encounter a multitude of problems. The condition affects every normal function of the face except vision1. The defect creates difficulty in feeding, breathing, hampers the facial growth, dentition and speech. It also creates social and psychological problems which have an impact on the child and parent2. The difficulty with feeding becomes a major concern which is mainly due to insufficient weight gain affecting the growth and development of the child. There is also risk for aspiration and associated complications in cleft palate cases.
Most of the children with cleft palate defect are unable to be breastfed as they cannot create the negative pressure required for suckling3-7. The surgical corrections for rectifying the clefts are deferred until the child is 3 months of age or older; the palatoplasty is performed even later, usually between 6-12 months of age2. A feeding obturator is a prosthetic device that helps to restore the separation of oral and nasal cavities, providing a rigid platform onto which baby can press the nipple and extract milk3,7. It restores the basic functions until the surgical corrections of the defects are completed. The article presents a case report of a neonate with unilateral cleft lip and palate for whom a feeding obturator was delivered.
A 5 days old healthy baby boy presenting with orofacial cleft and resultant feeding disability was referred to department of Prosthodontics, PMS Dental College of Science and Research, Trivandrum. The medical history of the child and parents was noncontributory. On examination, (Figure 1) the child was found to have unilateral cleft lip and palate (Veau classification, Class III). As the surgical correction of lip and palatoplasty were not scheduled for the near future, it was decided to construct a feeding plate obturator for the child.
The impression of the maxillary arch was made with low fusing impression compound? (Asian Acralyn Impression compound Aslate). The baby was held with his face facing the floor and the baby was crying during the procedure., ensuring the airway was patent throughout the procedure. (Figure 2)
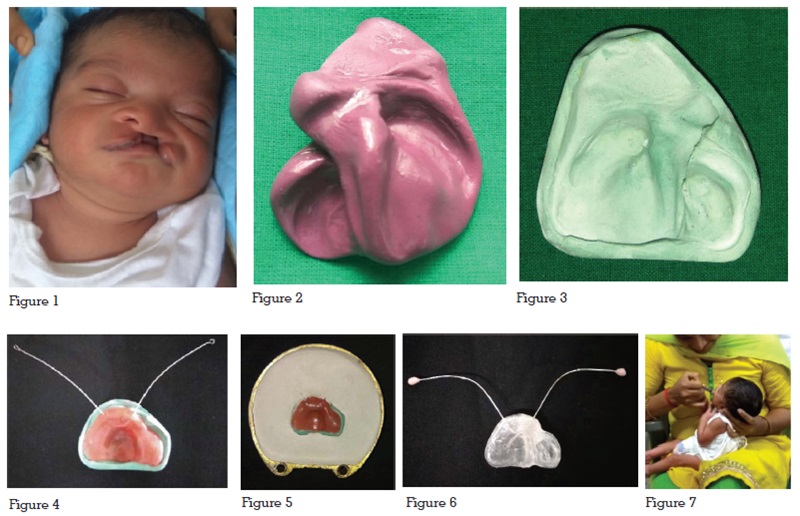
The impression was poured in Type III dental stone. The cast was thoroughly examined and rough surfaces were smoothened with emery paper (Figure 3). A wax sheet was adapted over the cast covering the defect. A 20-gauge wire was adapted on to the anterior part as shown in Figure 4. This was done to prevent accidental aspiration of the obturator as well as to facilitate easy handling of the prosthesis during insertion and removal.
Flasking, de-waxing was done and feeding plate was fabricated with heat activated clear acrylic. Small acrylic buttons were added to the tip of the wires to cover the sharp ends and avoid injury. (Figure 5-6). After trimming finishing and polishing the obturator was tried in patient’s oral cavity. The patient was fed in the dental clinic. There was no nasal regurgitation and the suckling could be clearly appreciated. (Figure 7). The parents were given instructions regarding the usage and maintenance of the appliance. The patient was reviewed after 24 hours and then on a monthly basis. The prosthesis was refabricated after 3 months following the surgical correction of upper lip. The neonatal weight gain and general health were closely monitored during the follow up visits.
The rehabilitation of orofacial clefting demands a multidisciplinary approach involving the dental team (Pedodontist, Prosthodontist, Orthodontist, Oral Surgeon), Pediatrician, Plastic Surgeon, Otolaryngologist, Psychologist and Speech Therapist. Primary care is crucial in these patients, who often have various health care needs, including feeding difficulties, speech correction, chronic ear infections and dental problems. The pre surgical management of orofacial cleft defects should begin as early as possible after birth8.
A wide variety of devices are available to aid in feeding infants with cleft defect such as: plastic squeeze bottles, feeding bottles with specially designed nipples (soft nipple, nipples with enlarged opening, wide base, long nipple). The feeding obturator prosthesis aids in positioning the tongue in position, reduces nasal regurgitation and choking, thereby considerably reduces the feeding time. Special care has to be taken while feeding infants with cleft defect. The age of the patient, size constraints and the anatomical variation are the main challenges in the fabrication of the prosthesis9.
It is advised to massage the breasts and apply hot packs 20 minutes prior to nursing. The mother has to apply finger pressure on the areola, to help protrude the engorged nipple, which will help the infant easy to hold on to the nipple. The infant should be held in a semi upright/straddle position/modified football hold; this prevents the milk from leaking into the nose and causing the infant to choke. The breast should be supported by holding it between thumb and middle finger. While nursing the infant’s tongue should be under the nipple and lower lip turned out1,10.
Strict follow up is an absolute necessary for patients using feeding obturator prosthesis. The obturator has to be refabricated as the child grows until the surgical correction is completed.
A feeding obturator prosthesis effectively overcomes the obstacles in the normal developmental milestones in a child with cleft defect. It aids in nursing, orofacial development, brings down the number of ear infections along with being a psychological help to the parents.