In long term edentulous patients, inadequate retention and stability of a complete denture are often encountered. Among the various reasons the presence of flabby tissue complicates the situation. This case report describes the design, fabrication and use of a fluid retained denture in a patient with completely edentulous maxillary and mandibular arch with flabby tissue in maxillary anterior and posterior region. The problem with conventional denture is rigidity of tissue surface, leading to uneven distribution of load. This worsens in the case of flabby, atrophic and unemployed ridges with excessive bone resorption. A Liquid supported denture allows uniform stress distribution due to its flexible tissue surface and provides improved patient’s acceptance.
A flabby ridge is an area of movable soft tissue in the maxillary or mandibular ridges. It is a common finding in long term denture wearers and may develop when the alveolar bone is replaced by soft tissue.1,2 Muscle dynamics or tissue irritation can cause soft tissue changes and bone resorption and this ultimately affects the residual ridge dimensions. In a flabby ridge condition, the denture base should be flexible so that it can adapt to the mucosa whenever necessary. However, the teeth need support for function in which case it also has to be rigid.3 Presentlyno one material exists which can combine both these properties nonetheless, with a mixture of materials, the base can be made rigid wherever it has to be sturdy and flexible once in contact with the soft tissues.
The utilization of elastic impression material to relieve traumatized tissue was introduced by Chase in 1961. However, this proved to be a temporary provision and as it was also prone to promote candidal growth4. Soft liners are another group of materials which have been used to relieve denture sore mouth. The essential difference between tissue conditioners and soft liners is that because the latter is plastic, it flows continuously under masticatory forces; until finally no material remains5. However soft liners also are solely temporary provisions as they lose their plastic properties due to the loss of plasticizer over a period of time.
In a flabby ridge condition stress concentration and trauma on the underlying tissues are an area of concern and hence the denture should be flexible. On the other hand, masticatory forces should be withstood by the denture tissues.2 Literature suggests that a prosthesis with a provision for incorporating a liquid within would be a solution to such clinical situations so that the design can combine characteristics of plasticity and elastic recovery.
This article describes the design of a maxillary complete denture with its base covered with a close fitting and flexible sheet containing a thin film of viscous liquid.
A 60-year-old female patient reported to PMS College of dental Science and Research, Vattappara, Trivandrum for replacement of missing teeth. The patient has been a complete denture wearer for 15 years. Her chief complaint was the poor fit of the denture and that it felt loose while eating. (Figure 1, 2) She was also using denture adhesive. On intraoral examination, a completely edentulous maxillary arch and mandibular arch with flabby tissue existing in the maxillary anterior and posterior region were observed. (Figure 3, 4) Treatment options given for this patient were implant retained prosthesis or conventional prosthodontics without surgical intervention. Considering the varied challenges related to the case, clinical steps and finance of the patient it was determined to give a maxillary liquid supported complete denture opposing a mandibular conventional complete denture.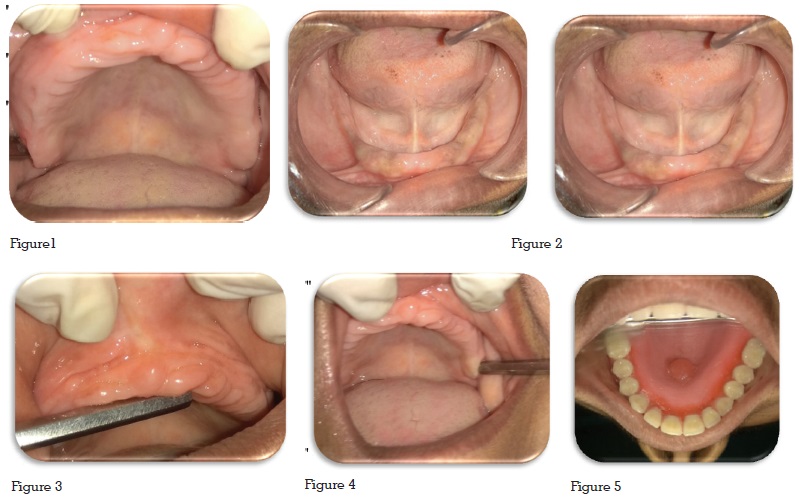
The primary concern in this case was the presence of movable tissue in anterior and posterior maxilla. This might have resulted in an unfavorable distribution of masticatory forces. Liquid-supported denture is based on the concept that when the force applied on the denture is absent, the base assumes its pre-shaped form and on application of force, the base due to the hydrodynamics of the liquid lining, adapts to the modified form of mucosa, improving support, retention and stability.3
The prime benefits of the liquid-supported denture includes6:
When no forces are applied, the foil remains in the resting position, acting as a soft liner and when the dentures are in use, vertically directed loads are distributed in all directions by the liquid resulting in optimal stress distribution.7
The liquid-supported denture is indicated in severely resorbed maxillary and mandibular ridges, inflamed or flabby tissues, vesiculo-bullous lesions like pemphigus, pemphigoid, erythema multiforme, oral lichen planus, and patient with systemic disorders like diabetes mellitus.8
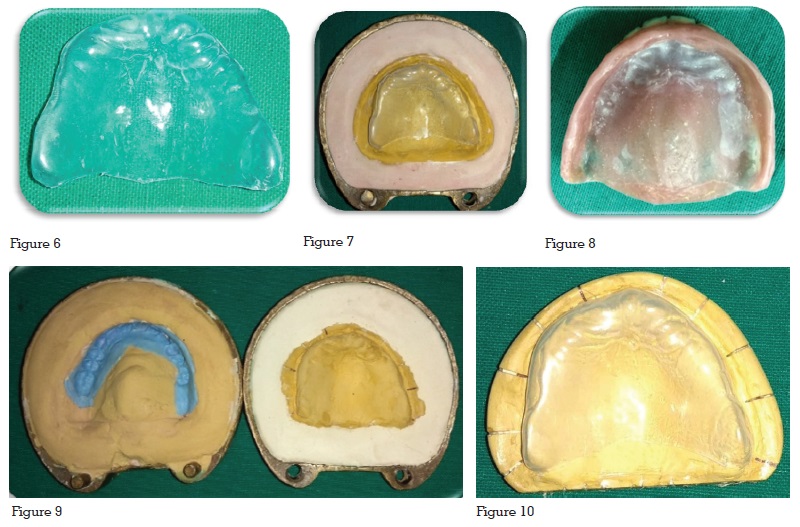
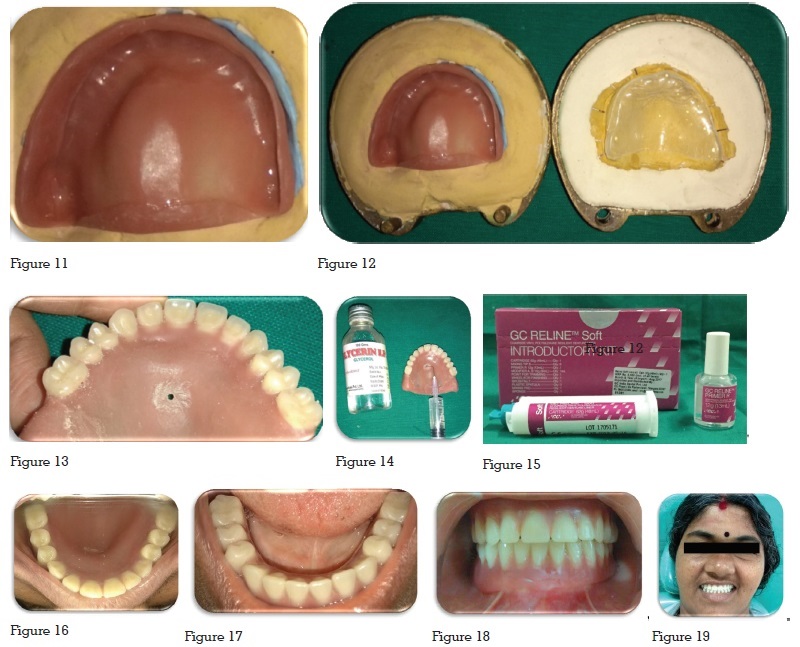
Due to its softness, flexibility and biocompatibility, polyethylene thermoplastic clear sheet was used. The liquid used was glycerin because of its clearness, viscosity and biocompatibility.
Earlier the problem faced in fabrication was difficulty in achieving complete seal at the junction of polyethylene sheet and denture base. This was overcome by flasking the denture once again before autoploymerizing resin was used. The main drawback is relining is not possible in fluid retained dentures.
Flabby ridges, often, causes difficulty in retention and stability of the denture bases and poses a real challenge to a prosthodontist for achieving the basic objectives of impression making. Surgical intervention and implant-supported dentures may not be possible to be applied in all those clinical conditions. Liquid supported denture offers a solution in such situations while considering conventional prosthodontics. This concept can further improve the patient’s comfort and acceptance due to more uniform distribution of occlusal forces.