Periodontitis is an inflammatory disease which manifests clinically as loss of supporting tissues and leads to tooth loss .Though implants are an ideal way to replace a missing tooth, still lacking is the presence of the periodontal ligament, as in the natural teeth. A tissue-engineered periodontal ligament (PDL) around implants would represent an important new therapeutic tool to replace lost teeth. The PDL is the key to tooth anchoring; it connects tooth root and alveolar bone, and it sustains bone formation. Cells were isolated from PDL and cultured in a Bioreactor on titanium pins. Thus,Implants with PDL may be installed in the extraction socket of the missing tooth, thereby facilitatingthe surgical procedure.
Key words: Periodontal Ligament,Tooth implant, Tissue Engineering, Bioreactor, Osseointegration, Cell Culture
Bone resorption following tooth loss can lead to a significant decrease in alveolar bone height, thereby compromising subsequent implant placement and long-term stability.1
Dental implants are nowadays the treatment of choice to replace missing teeth due to their high predictability and long-term success. This success is the outcome of several cellular and molecular events that take place at the implantbone interface2. Despite the high success rate of dental implants, complications have been reported such as implant prosthetic screw fracture, fracture of implant abutment screws, infection, prolonged bleeding, damage to other teeth, delayed bone healing, jaw fracture and many others.3
Many strategies to improve the osseointegrative property of the implant have been documented; these include surface treatments of implants to improve mechanical, physical, and chemical characteristics of implants or altering surface topography to control cell behavior. Addition of biomimetics (growth factors) to the implant surface also proved beneficial.4
Tissue-engineering has emerged as a new and ambitious approach that combines knowledge from material chemistry with cell biology and medicine. These strategies used biodegradable polymers to make scaffolds into the cells were inserted to produce tissues in the presence of growth factors. The first generation of tissue engineering can be used for constructing cartilage or bone. The second generation of tissue engineering requires a new method of tissue reconstruction not based on scaffolds.5
Osseo- integrated implants are generally agreed to be the most acceptable implants because of their high long term clinical survival rate. The problems such as localized bone loss around the implant especially in case of Gingival recession, in addition these implants are ankylosed and do not have the same mobility as the natural teeth could be resolved by Ligaplants, which is nothing but combination of the PDL cells with implant biomaterial.6
Human periodontal ligament cells (Figure-1) were isolated from an extracted tooth. After extraction, periodontal tissue was scraped from the middle third of the root with a scalpel blade. The harvested tissue was placed into culture dishes containing Dulbecco’s modified Eagle’s minimal essential medium, supplemented with 10% fetal bovine serum and 100units/mL of penicillin- streptomycin. Then, those outgrowth cells were cultured in a humidified atmosphere of 5% CO2 at 37°C for 48 hours to allow attachment of the cells to the dishes. The dishes were washed to eliminate debris and the medium was changed three times per week. To harvest the cell sheet, human periodontal ligament cells were plated on temperature- responsive culture dishes (35 mm in diameter) at a cell density of 1x105 and cultured at 37°C supplemented with 50mg/mL ascorbic acid 2- phosphate,10nM dexamethasone and 10nM ß- glycerophosphate that function as an osteodifferentiation medium.6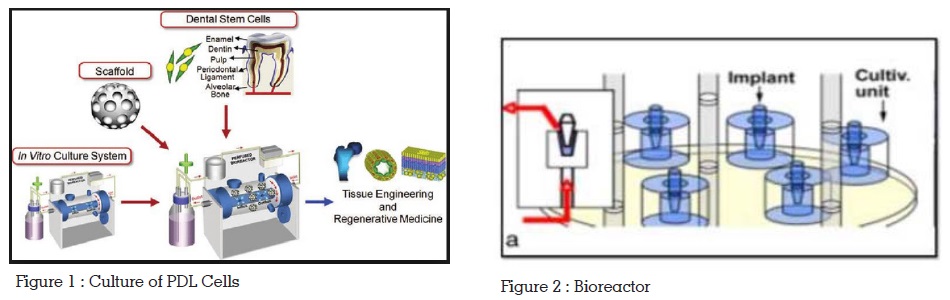
N- isopropylacylamide monomer in 2- propanal solution was spread onto polystyrene culture dishes. Then the dishes were subjected to electron beam irradiation with an Area Beam Electron Processing System. The temperature- responsive polymer- grafted (poly N isopropylacrylamide) dishes were rinsed with cold water to remove ungrafted monomer and sterilized with ethylene oxide.6
A titanium pin, which coated with Hydroxyapatite (HAP), was placed in a hollow plastic cylinder leaving a gap of 3mm around the pin. Culture medium was continuously pumped through the gap. Single cells suspension, obtained 3mm around the pin. Culture medium was continuously pumped through the gap. Single cells suspension, obtained from human, was seeded first into plastic vessels under a flow of growth medium for 18 days (Figure-2). cells are positioned in a narrow space between the ligaplant and surrounding hollow cylinder. It was thereby anticipated that the PDL phenotype would be favoured implicating a tight attachment of cells to the implant. So,the preparation of the ligaplants should have instantly mechanical movements of the medium flow and space between the implants and the culture should be optimal and the duration of the surface treatment should also be optimal to obtain the successful ligaplants which brings big improvements to the implant system.6
Tooth transplantation with double PDL stimulation is one of the best examples of its healing capacity. Fourteen days before transplantation, the donor tooth is extracted and immediately replanted in its original alveolus. This deliberate trauma triggers a healing process within the PDL, which includes cell proliferation and differentiation. The in vivo cell culture reaches its peak of activity after 14 days, after which the transplantation of the tooth can be performed with millions of cells full activity attached to its root by new Sharpey’s fibres.
Using this model in its biological and clinical aspect, we now use similar cell culture around an artificial root using tissue engineering techniques.6
Nowadays, fixed and removable partial dentures are replaced by implants, which holds ideal for replacing missing tooth. For implant to be successful, factor such as sufficient bone [height and width] is very crucial. Before placement of the implant, local bone defects and generally poor bone quality necessitate bone reconstruction. Besides that, localized bone loss around the implant fixture represents the clinical challenge especially in the case of gingival recession, which requires further surgical interventions. However, problems still exist with these implants as they lack PDL, because any inflammation around them may cause serious bone loss than does the inflammation around the natural tooth with PDL. In addition, these implants are ankylosed and do not have the same mobility as the natural teeth.6
The implants are being placed with the aim of attaining osseointegration without giving consideration to the regeneration of periodontium around the implant. The boom in implant dentistry is attributed to a combination of various reasons; prolonged life span of aging individuals, failures associated with removable and fixed prostheses, advantages and predictable outcomes associated with the use of implants.4
The description of the process of osseointegration by Brånemark et al., dental implants have become ideal replacements for missing teeth. The term osseointegration was later defined by Albrektsson et al. as the direct contact between living bone and implant at the light microscope level. This means that the implants are functionally ankylosed to the bone without periodontal ligament support. However, despite good success rates of osseointegrated oral implants, failures do occur, which can be attributed to the bone loss due to excessive occlusal load and/or infection.3 Hence, the focus of implant dentistry has changed from merely obtaining osseointegration to the preservation and prevention of peri-implant hard and soft tissue loss. Currently, lost teeth are being replaced by implants made of inert biomaterial, which are directly inserted into the alveolar bone to achieve osseointegration without considering the regeneration of periodontium. The field of oral and periodontal regenerative medicine has recently undergone significant advancements in restoring as close as possible the architecture and function of lost structures. To date, a major “disconnect” exists between the principles of periodontal regeneration and oral implant osseointegration. That entity is the presence of a periodontal ligament (PDL) to allow for a more dynamic role beyond the functionally ankylosed or osseointegrated oral implant. Therefore, an innovative approach is mandatory to create “periodontio-integrated implants” i.e., an implant suspended in the socket through periodontal ligament as opposed to functionally ankylosed osseointegrated implants.4 The authors of the present study believe that such advancement would revolutionize implant dentistry and would be significantly beneficial to patients.
However, sometimes the absence of movement of the implant can cause build up of forces and drastically harm the quality and quantity of the surrounding alveolar bone, implant as well as the TMJ.4
Though implants are an ideal way to replace a missing tooth, still lacking is the presence of the periodontal ligament, as in the natural teeth. This soft, richly vascular, and cellular connective tissue permits forces, elicited during masticatory function and other contact movements to be distributed to the alveolar process via the alveolar bone proper. It acts like a shock absorber, giving the tooth some movement in the socket. It also provides proprioception. The periodontal ligament also has an important interaction with the adjacent bone, playing the role of the periosteum, at the bone side facing the root. It homes vital cells such as osteoclasts, osteoblasts, fibroblasts, cementoblasts, cementoclasts, and most importantly, the undifferentiated mesenchymal stem cells. These cells are all important in the dynamic relationship between the tooth and the bone.4 Therefore, strategies to generate dental implants with associated periodontal tissues have become a new approach in tooth replacement therapies.
As early as 1990, Buser et al. showed that titanium dental implants when placed in contact with retained root tips, the periodontal ligament of these roots served as a source for cells which could populate the implant surface during healing. Now, tissue engineering has opened a new vista in periodontal regeneration and more so in the treatment of dental implants. From various scaffolds to matrices, all have proved their ability to regenerate the entire periodontium.4
The periodontal ligament is the soft connective tissue interposed between the roots of the tooth and the inner wall of the alveolar sockets. Apart from its role in the tooth anchoring, the periodontal ligament (PDL) provides progenitor cells for alveolar bone formation and remodeling; and it plays the role of the periosteum in the alveolar socket that faces the root of the tooth. Periodontitis is characterized by the destruction of tissues, such as alveolar bone, cementum and the periodontal ligament which may be followed by tooth loss. A possible approach to the replacement of tooth loss is tissue engineering of the PDL. As the PDL has been shown to possess a capacity for spontaneous regeneration, during which the biomechanical tissue strength is restored and innervations is re-established.5
Ligaplant is a new application of tissue engineering and a developing area for clinicians and researchers. New tissue consistent with PDL developed on the surface of dental implants after implantation has decisive advantages as compared with osseointegrated oral implants, due to their periodontal tissue degeneration. Besides that,patient may not have to undergo bone grafting, inconvenience and discomfort with the Ligaplant placement. The implants with tissueengineered ligament definitely score over the current implant scenario and are going to be the future in implant dentistry. Since most of these studies are carried out in animals and has been revealed that generating a periodontal-like tissue around implants is possible, still a predictable and feasible method for producing dental implants with periodontal-like ligament has not been innovated and more studies are required in clinical especially in humans in order to know its long term stability, function,survival and success of these implants.6