The post extraction ridge changes, in hard and soft tissues, poses challenging situation to the restorative and implantologist1. A variety of ridge preservation techniques using tissue and augmentative materials have been proposed in the literature along with extraction of complete root and immediate implant placement with immediate provisional prosthesis2,3. In recent years, another technique known as Root Membrane Technique has gained popularity as a treatment of choice for rehabilitation in esthetic zone4. The present case report provides a comparison of two different techniques of rehabilitation in esthetic zone in the same patient.
Key words: alveolar bone preservation, extraction socket, immediate implant placement, socket shield, tooth retention, post-extraction, esthetics
The extraction of teeth is inevitably associated with
definitive changes in the surrounding hard and soft
tissues. After tooth extraction, the alveolar bone
undergoes a remodelling process, which leads to
horizontal and vertical bone loss. These resorption
processes complicate the prosthetic rehabilitation of the missing tooth. Various methods of hard and
soft tissue grafting procedures are required to
regain the original dimension of the bone after
extraction. These procedures require additional
training and high level of surgical skills on the
behalf of the clinician.
The increased esthetic demand leads to the need
of a successful treatment option with a short course
and need of an alternative treatment option to
avoid the grafting procedures. This has drawn the
attention towards the use of immediate implant
placement with immediate or early loading5. This
option not only eliminates or reduces the healing
period of conventional implant therapy, but the
patients can return to their normal daily life with
provisional or definitive prosthesis attached over it.
Immediate implant placement and loading have
shown a high success rate of 95% - 98% when
proper case selection and surgical protocol is
followed6. Immediate implant placement has
shown to minimized treatment failures but it cannot
prevent the resorption of the bundle bone which
lies on the socket side of buccal bone. In case
where there is very thin buccal bone, resorption
of bundle bone leads to controlled but evident
horizontal and vertical bone loss of buccal bone
even if immediate implant placement is done7.
The resorption of the buccal bundle bone can be prevented only by leaving a buccal root segment
in place, which retains the periodontal ligament,
the lamina dura and the periodontal vascular
supply of the buccal bone8. This way the biological
integrity of the buccal periodontium (bundle bone)
remains untouched. This method, popularly known
the Root Membrane Technique (RMT), has also
been described in connection with immediate
implant placement3,9.
The RMT involves the retention of the facial or
buccal root section alone to preserve the buccal
bone and overlying soft tissues at the time of an
immediate implant placement. A tooth planned for
extraction with immediate placement is sectioned
mesiodistally such that the facial and palatal root
halves may be separated. The palatal root section
is then extracted atraumatically, leaving the facial
root section to remain in situ. The root section is
carefully shaped and prepared using long shank
round burs. With an implant is placed palatal to
the prepared root membrane. The root membrane maintains the attachment to bundle bone and its
vascularity, and the support of the ridge facial to
the implant and the restoration9.
There are very few studies which compare these
two different techniques of immediate implant
placement; one with RMT and one without RMT.
These studies have data from different patients and
different age groups. The case report documented
here is a unique and rare case report as the two
different techniques are done in the same quadrant
of one patient and were done at the same time by
the same clinician.
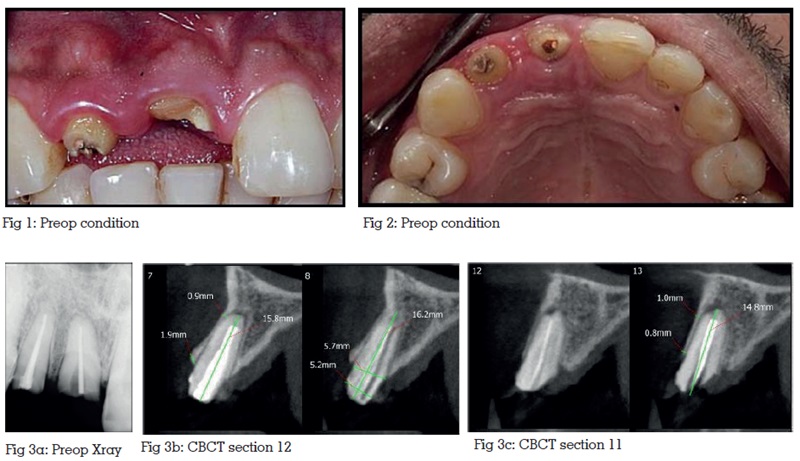
A 24-year-old, healthy male patient with fractured right lateral and central incisor presented with a chief complaint of repeated decementation of crowns in relation to right lateral and central incisors. As the concerned teeth were in esthetic zone; patient wants to have permanent and quick solution to his problem. Clinical examination of #11, #12 revealed that the tooth structure was insufficient for fabrication of post and core and new crowns (Fig 1, 2). Immediate implant placement with RMT and immediate provisionalistion in both the incisors was chosen as treatment modality and was discussed with the patient. A detailed dental and medical history was taken. The patient was a non-smoker and did not present relevant medical conditions. Radiographic examination revealed root canal treated #11, #12 with no sign of periapical infection (Fig. 3a). CBCT evaluation confirmed presence of very thin buccal bone in relation to both the incisors (Fig 3b, Fig 3c).
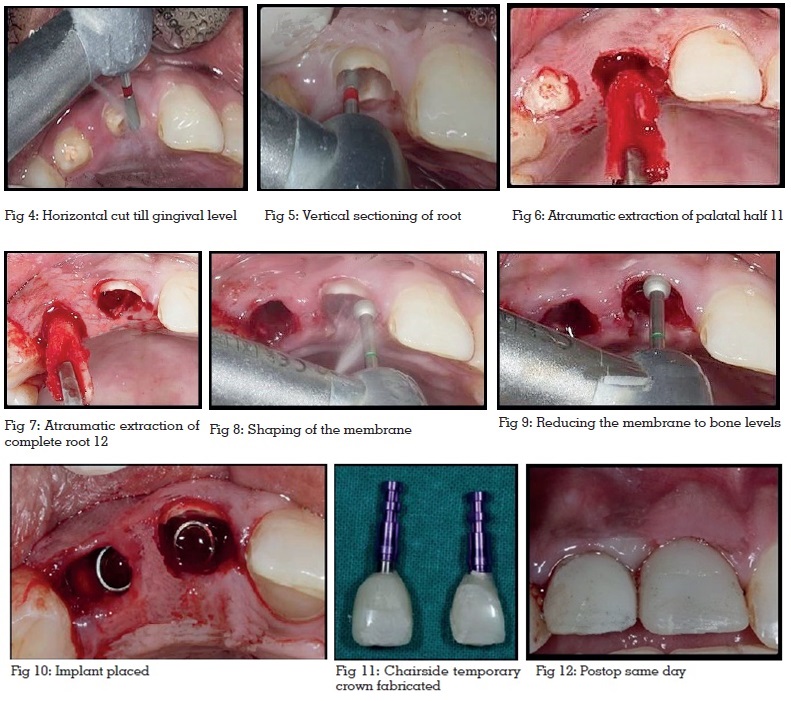
After the local anaesthesia was achieved, both the teeth were carefully decoronated using a diamond bur (Fig. 4). The teeth were carefully bifurcated into buccal and palatal parts using a long shank diamond bur (Fig. 5). Particular attention was taken to avoid damage to the buccal bone. It’s important to confirm the complete separation of the buccal and palatal parts before any periotomes or luxators are used. This can be done using a long tip straight probe. The palatal part was then carefully extracted using periotomes and luxators as traumatically as possible. The palatal root of #11 was successfully extracted out of the socket (Fig. 6) but when the same procedure was tried in #12, the buccal part of the root became mobile. The mobile root piece cannot be left in the socket; hence both the buccal and palatal part #12 were extracted (Fig. 7). The buccal fragment of the root of #11 was carefully shaped using a long shank round bur in such a way that the thickness of remaining segment was around 2mm and it is 1mm coronal to the buccal bone plate (Fig. 8, 9). The coronal part of the shield was shaped so that it slopes towards the socket; this preparation allows enough room for the correct form and shape of the prosthesis without the prosthesis touching the shield.
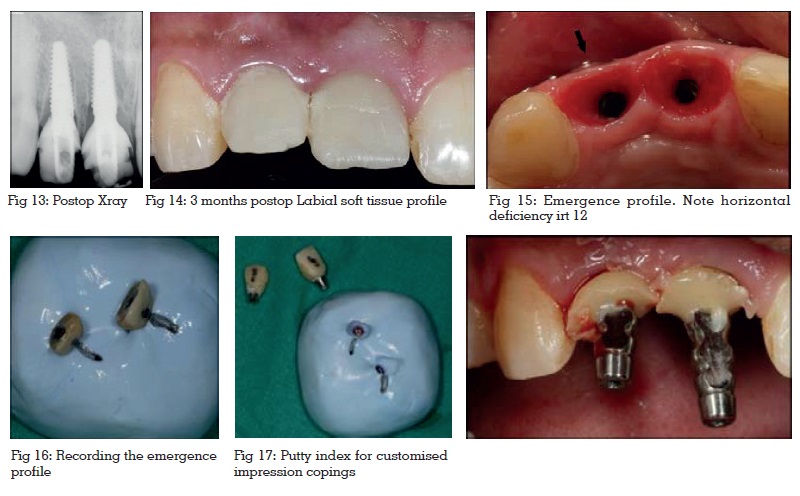
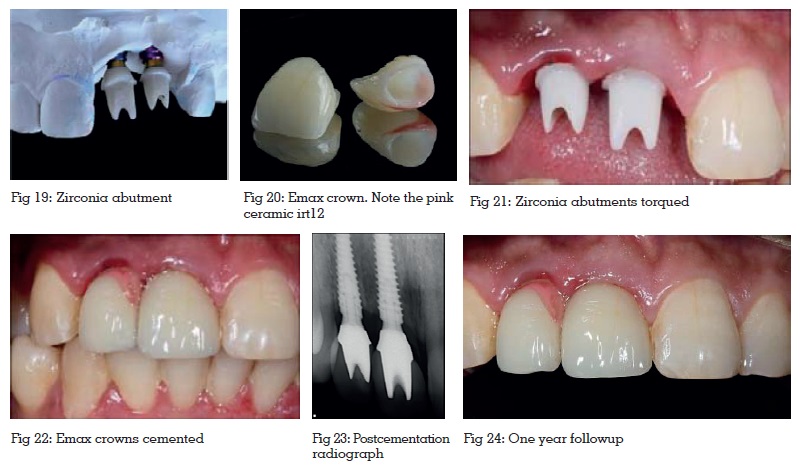
A careful curettage of the extraction socket was performed to remove granulation tissue. Preparation of osteotomy sites was carried out; in the palatal part of both the sockets; using the sequential order of calibrated drills recommended by the manufacturer. The implants (Megagen Any Ridge) were placed according to the manufacturer’s recommendations avoiding contact within #11 retained root fragment (Fig. 10). High insertion torque values indicated good primary stability. Straight titanium cylinders provided by the company were used for temporisation and chairside temporaries were fabricated. Special attention was paid to the emergence profile of the provisional implant crown. At the sub gingival portion, an S-shape was designed to avoid placing any pressure on the root fragment (Fig. 11). The temporary crowns were kept out of contact in centric as well as all eccentric contacts to avoid functional loading on the implants (Fig.12, 13). 3 day, 7 day and 15 day follow-up examinations were done. The implant site showed uneventful healing. The patient was called after three months for the final restorations (Fig.14). When the temporary crowns were removed, a very nice and healthy gingival emergence profile was seen (Fig.15). No membrane exposure was observed. There was buccopalatal collapse of gingival tissue in #12 regions where no root membrane was present. Contrary to this gingival profile in #11 region with a root membrane had a buccal convexity in the same way it had before the surgery. In addition to this, it was also observed that there was some vertical loss of bone and soft tissue in #12 region resulting in longer crown. The submucosal emergence profile of the provisional implant crowns were recorded (Fig. 16,17) and transferred into the final restoration using customised impression copings (Fig. 18). The final restorations, E-max crown on Zirconia abutments, were delivered four months after implant placement (Fig. 19, 20, 21). Perfect pink and white esthetics was achieved in the right central incisor region which had a root membrane inside. On the contrary right lateral incisor region; where there was no root membrane, a vertical and horizontal soft tissue loss was noticed, hence pink ceramic was used to maintain the pink white balance and to achieve esthetically pleasing results (Fig. 22,23). A one year follow-up was done and the gingival levels were found to be absolutely healthy and stable (Fig. 24).
The ideal technique for restoring a grossly mutilated and non restorable tooth should be simple, minimally invasive, and be able to preserve the attached gingiva and soft tissue contours. Moreover, this should be achieved with minimal surgery. Ridge atrophy is a major culprit in the creation of esthetically unfavorable outcomes especially in the maxillary anterior region. Retaining the gingival contour is one of the most significant factors in the esthetic rehabilitation of the maxillary anterior region. The root submergence technique (RST)8 was introduced to preserve the alveolar ridge; later it was used to prevent down growth of epithelium during the regeneration of periodontal tissues. The RST has served as a promising method of maintaining the dimensions of the alveolar ridge at the pontic site of a fixed dental prosthesis in the maxillary anterior esthetic zone but to use this site for implant placement needs a modification in the technique. This modification came to be known as Root membrane Technique or RMT4 in which only a part of the root was retained while the remaining part of the socket was used for the immediate implant placement. This has added benefits of preventing the buccopalatal collapse of the labial plate seen most commonly after the conventional immediate implant placements which are done after the extraction of the complete root fragment.
Immediate implant placement does not stop the process of socket and ridge remodelling because the implants can never surpass the natural tooth’s ability to preserve the surrounding bone and soft tissue height. Clinicians should therefore always consider to preserve the attachment apparatus of natural teeth that naturally and conservatively augments the shape of alveolar bone, as well as the gingival and alveolar mucosa; even if implant if placed immediately after the tooth extraction.
The studies7,9,11 done in the past advocates that the intentional preservation of the root membrane in the extraction socket, prior to the immediate implant placement, is a highly promising technique in terms of maintaining pink and white esthetics and provides a solution for esthetically critical cases like high lip line, maxillary anteriors etc. This technique not only preserves but also helps to maintain the hard and soft tissues, in future, as long as we have the intact shield.
The present clinical case presents a situation where a direct comparison of esthetics and soft tissue evaluation is done between two implants placed simultaneously in the same patient, immediately after the extraction one with RMT and other without RMT (RMT attempt failed because of mobility of the membrane).The clinical picture at the time of prosthesis clearly shows there is both vertical and horizontal resorption if tooth is removed in toto.
At the same time the limitations of the technique cannot be ignored. If the shield becomes mobile during surgery, it is removed and the conventional immediate implant placement or the grafting procedure is to be done. The case selection is very important for the success of the procedure. The technique is not recommended in periodontally involved teeth and teeth which are out of the arch.
The root membrane technique is gaining popularity amongst the clinicians across the world. It is a predictable therapy with minimum surgical intervention, less duration of total treatment and an optimum aesthetic result. However more studies are required to compare the results of the two different rehabilitation procedures so as to decide whether RMT is an essential treatment or an overtreatment modality. According to the current report it should always be considered as first line of treatment whenever rehabilitation of a tooth in an esthetic zone is considered.